






 Психология
ПсихологияПохожие презентации:







Mood Disorders
1.
Mood DisordersProf. Anatoly Kreinin MD, PhD,MHA
2.
О чем лекцияНастроение, аффект, расстройства настроения
• Нозология, эпидемиология, лечение
• Большое депрессивное расстройство (MDD)
• Стойкое депрессивное расстройство
• Предменструальное дисфорическое расстройство
• Деструктивное расстройство регуляции настроения
• Биполярное расстройство (BMD)
• Циклотимическое расстройство
3.
О чем лекция• Дифференциальный диагноз, в том числе:
• Депрессивное против биполярного расстройства и
связанные с ним расстройства, вызванные другим
заболеванием
• Депрессивное расстройство, вызванное приемом
психоактивных веществ/лекарств, против
биполярного и родственного расстройства
• Другое уточненное депрессивное v. Биполярное и
родственного расстройства
• Неуточненное депрессивное против биполярного и
родственного расстройства
4.
• Настроение - субъективное ощущение указывает надлительное, глубокое и постоянное чувство, которое влияет на
человека, его функционирование и окружающую его среду.
• Аффект - объективное впечатление врача или других лиц,
которое характеризует временную и кратковременную эмоцию,
наблюдаемую во время осмотра.
• Соответствует или не соответствует содержанию мышления
• Ситуация ...
• При нормальном настроении человек «перемещается» в
диапазоне НАСТРОЕНИЯ с разной степенью контроля.
• При расстройствах настроения – они контролируют пациента
5.
• Настроение - субъективное ощущение указывает надлительное, глубокое и постоянное чувство, которое влияет на
человека, его функционирование и окружающую его среду.
• Аффект - объективное впечатление врача или других лиц,
которое характеризует временную и кратковременную эмоцию,
наблюдаемую во время осмотра.
• Соответствует или не соответствует содержанию мышления
• Ситуация ...
• При нормальном настроении человек «перемещается» в
диапазоне НАСТРОЕНИЯ с разной степенью контроля.
• При расстройствах настроения – оно (Настроение)
контролирует пациента
6.
Отличие Настроение от Аффекта” Настроение» - устойчивое и длительное, по времени,
эмоциональное состояние, обычно оценивается и сообщается
самим пациентом.
«Аффект» - оценка и восприятие эмоционального состояния
пациента другими людьми.
Расстройства настроения
Психические состояния, при которых настроение является
основной, преобладающей проблемой
7.
Major Depressive Disorder8.
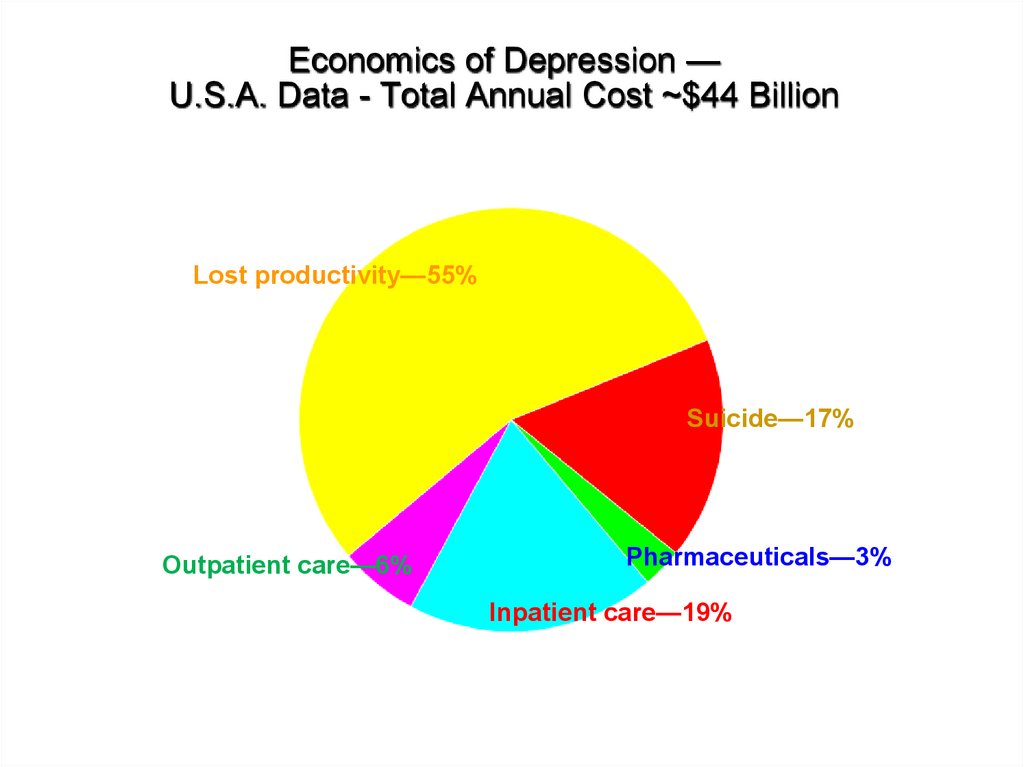
Economics of Depression —U.S.A. Data - Total Annual Cost ~$44 Billion
Lost productivity—55%
Suicide—17%
Outpatient care—6%
Pharmaceuticals—3%
Inpatient care—19%
9
9.
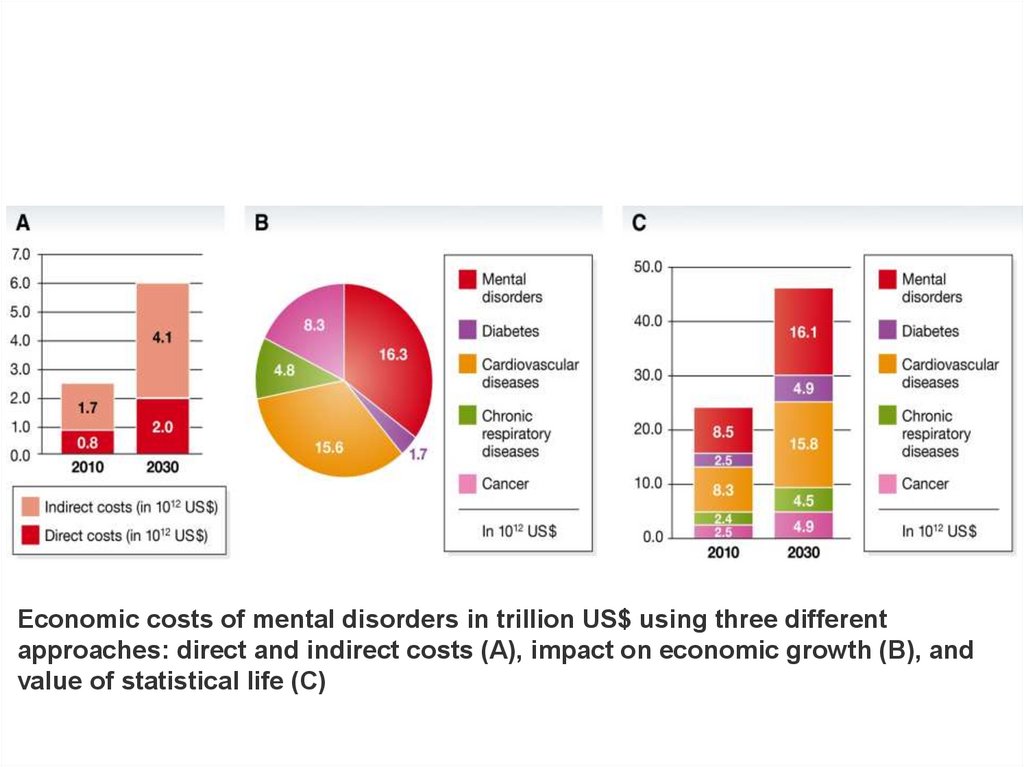
Economic costs of mental disorders in trillion US$ using three differentapproaches: direct and indirect costs (A), impact on economic growth (B), and
value of statistical life (C)
10.
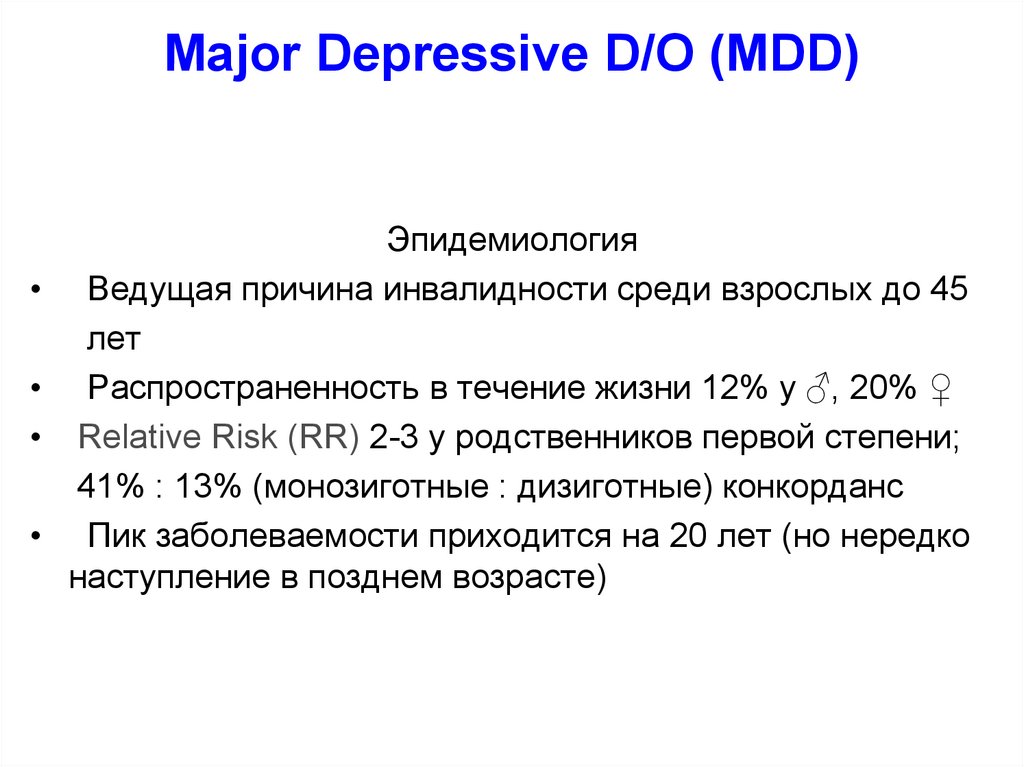
Major Depressive D/O (MDD)Эпидемиология
Ведущая причина инвалидности среди взрослых до 45
лет
Распространенность в течение жизни 12% у ♂, 20% ♀
Relative Risk (RR) 2-3 у родственников первой степени;
41% : 13% (монозиготные : дизиготные) конкорданс
Пик заболеваемости приходится на 20 лет (но нередко
наступление в позднем возрасте)
11.
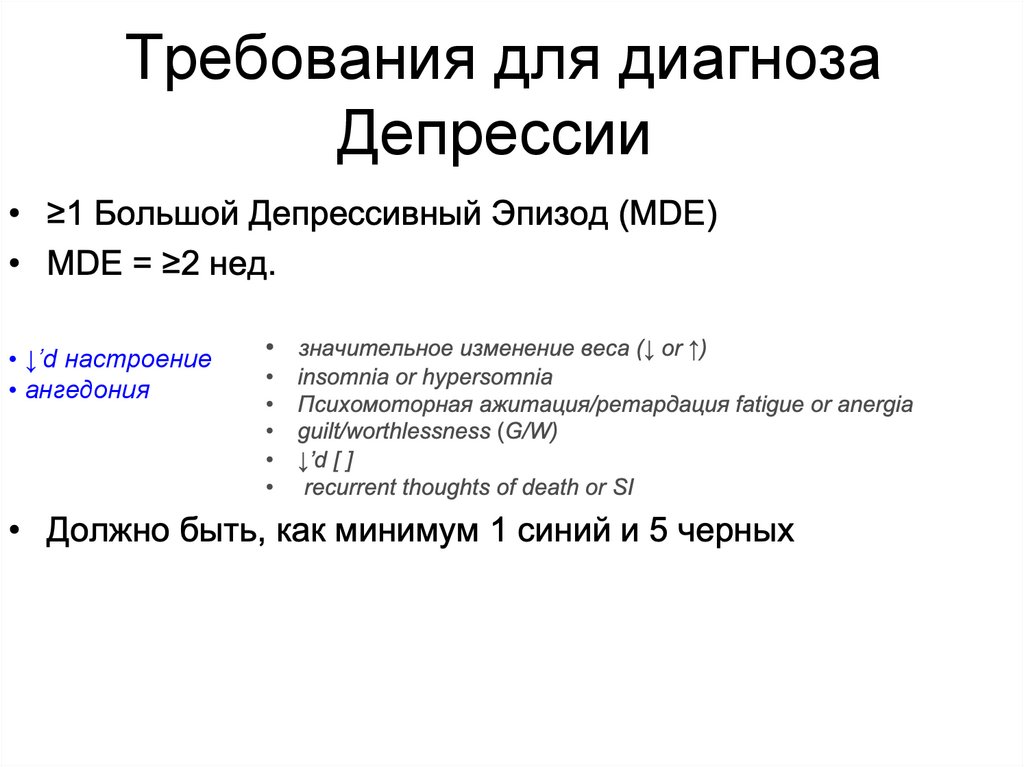
Требования для диагнозаДепрессии
• ↓’d настроение
• ангедония
12.
Question:Когда Большой Депрессивный Эпизод ≠ Большое Депрессивное
Расстройство?
ИСКЛЮЧЕНИЯ:
1. не вызвано веществом / лекарством или другим заболеванием
2. отсутствие предшествующих [эндогенных] эпизодов мании или гипомании
13.
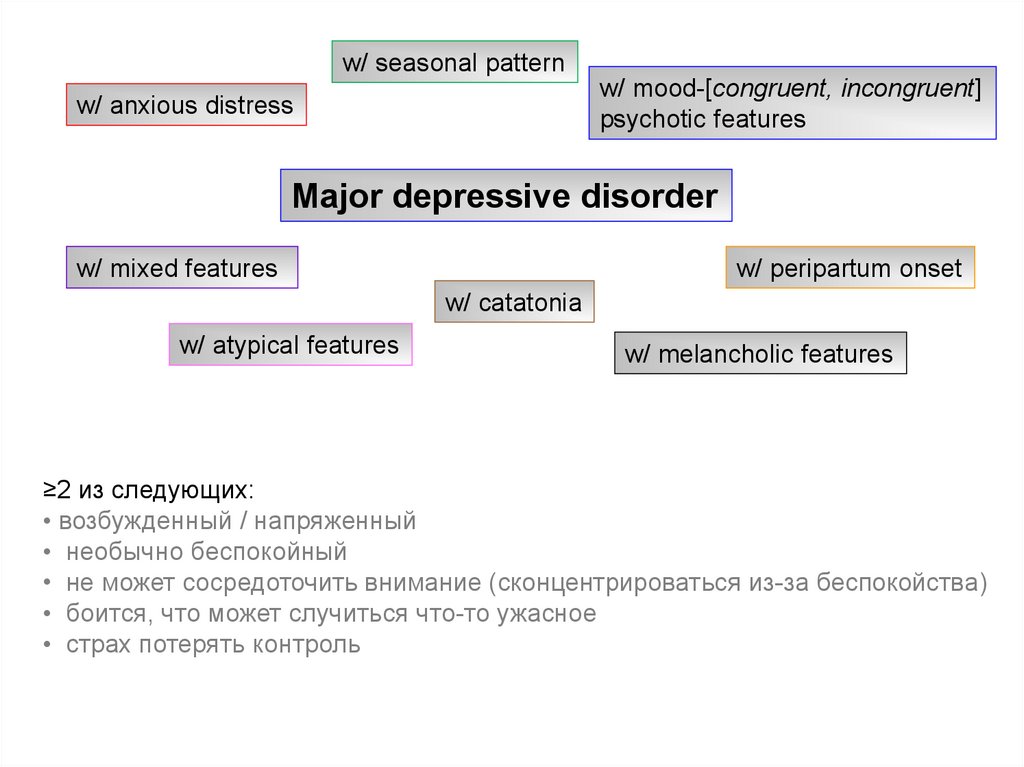
w/ seasonal patternw/ mood-[congruent, incongruent]
psychotic features
w/ anxious distress
Major depressive disorder
w/ mixed features
w/ peripartum onset
w/ catatonia
w/ atypical features
w/ melancholic features
≥2 из следующих:
• возбужденный / напряженный
• необычно беспокойный
• не может сосредоточить внимание (сконцентрироваться из-за беспокойства)
• боится, что может случиться что-то ужасное
• страх потерять контроль
14.
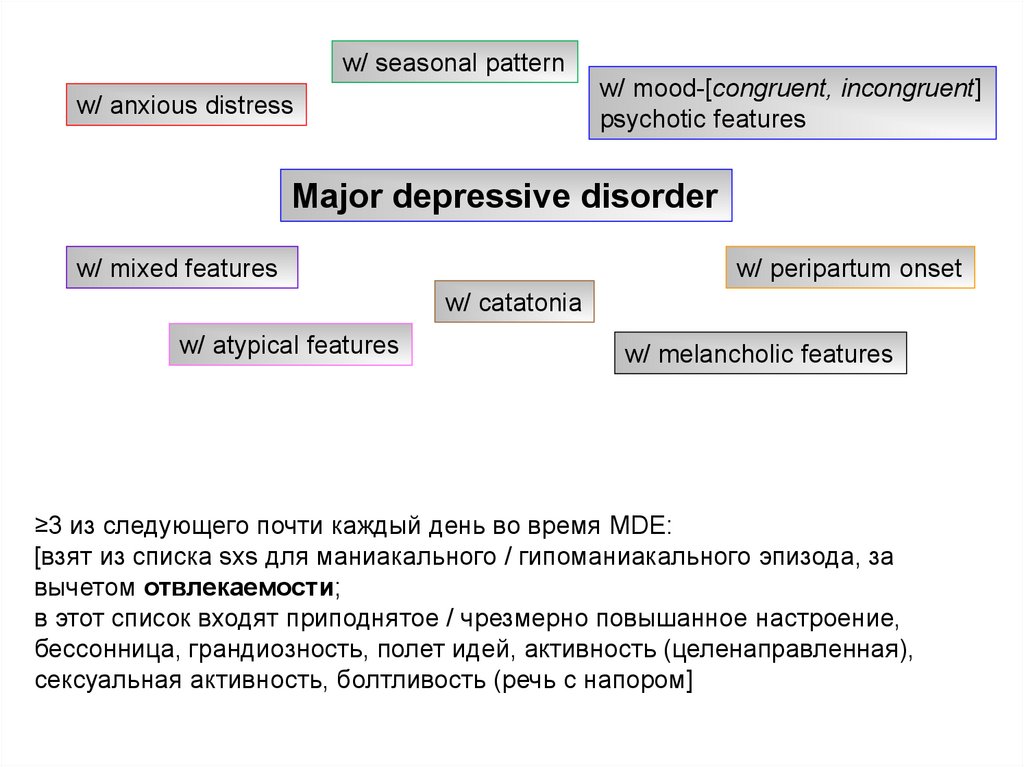
w/ seasonal patternw/ mood-[congruent, incongruent]
psychotic features
w/ anxious distress
Major depressive disorder
w/ mixed features
w/ peripartum onset
w/ catatonia
w/ atypical features
w/ melancholic features
≥3 из следующего почти каждый день во время MDE:
[взят из списка sxs для маниакального / гипоманиакального эпизода, за
вычетом отвлекаемости;
в этот список входят приподнятое / чрезмерно повышанное настроение,
бессонница, грандиозность, полет идей, активность (целенаправленная),
сексуальная активность, болтливость (речь с напором]
15.
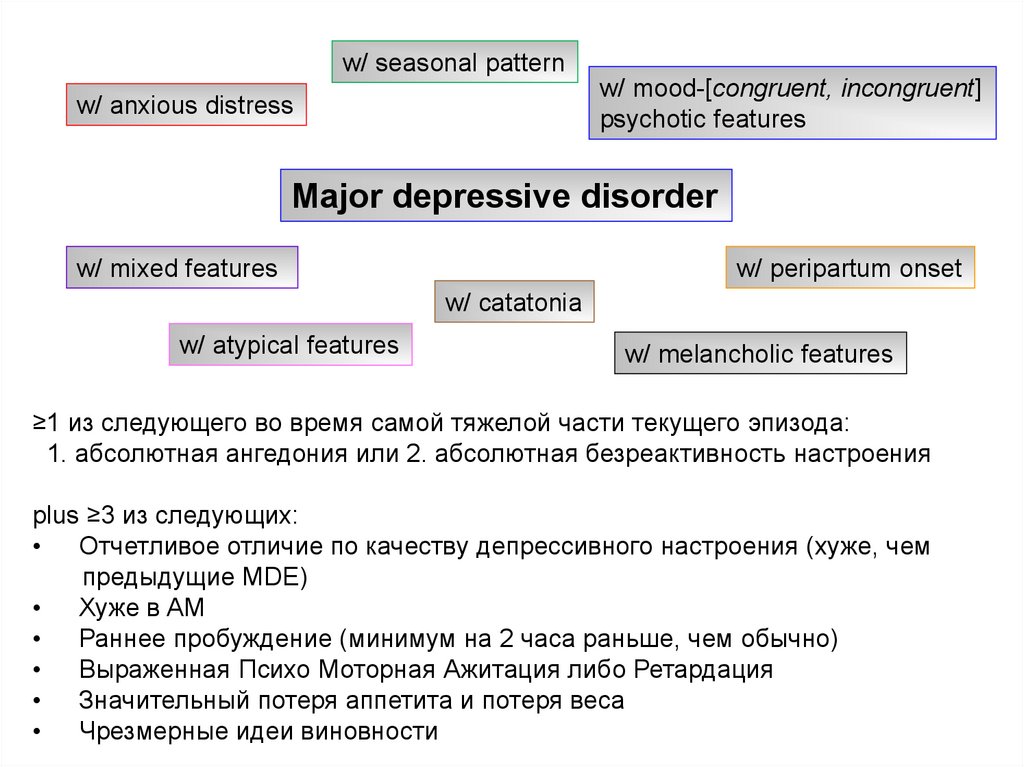
w/ seasonal patternw/ mood-[congruent, incongruent]
psychotic features
w/ anxious distress
Major depressive disorder
w/ mixed features
w/ peripartum onset
w/ catatonia
w/ atypical features
w/ melancholic features
≥1 из следующего во время самой тяжелой части текущего эпизода:
1. абсолютная ангедония или 2. абсолютная безреактивность настроения
plus ≥3 из следующих:
• Отчетливое отличие по качеству депрессивного настроения (хуже, чем
предыдущие MDE)
• Хуже в AM
• Раннее пробуждение (минимум на 2 часа раньше, чем обычно)
• Выраженная Психо Моторная Ажитация либо Ретардация
• Значительный потеря аппетита и потеря веса
• Чрезмерные идеи виновности
16.
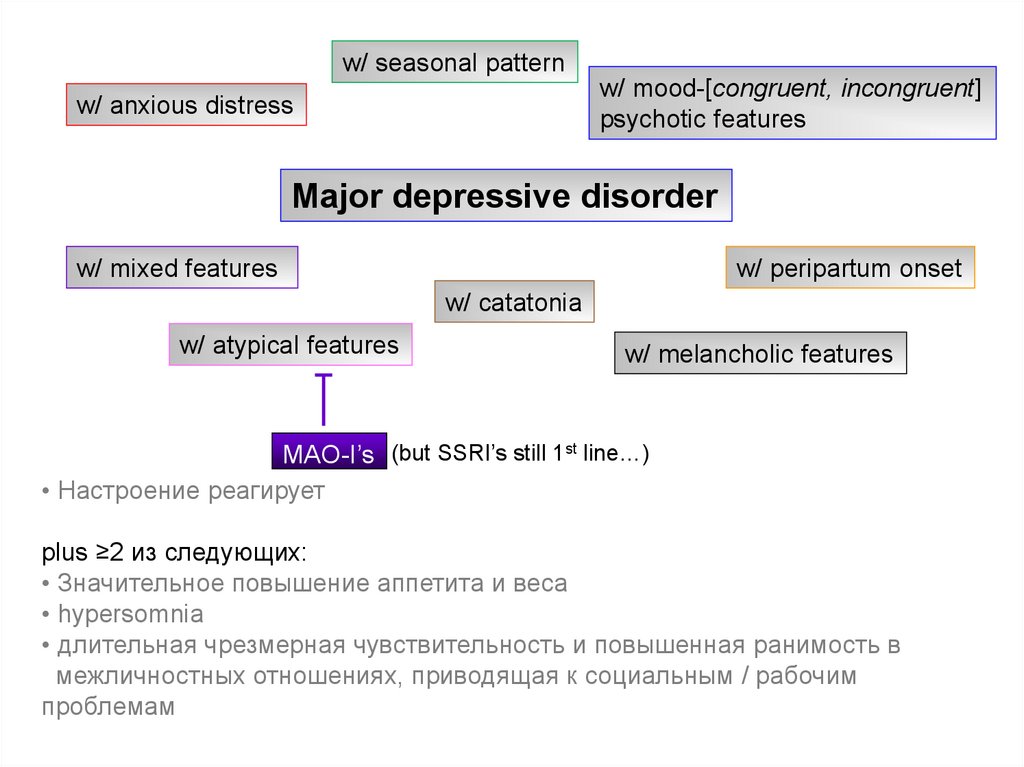
w/ seasonal patternw/ mood-[congruent, incongruent]
psychotic features
w/ anxious distress
Major depressive disorder
w/ mixed features
w/ peripartum onset
w/ catatonia
w/ atypical features
w/ melancholic features
MAO-I’s (but SSRI’s still 1st line…)
• Настроение реагирует
plus ≥2 из следующих:
• Значительное повышение аппетита и веса
• hypersomnia
• длительная чрезмерная чувствительность и повышенная ранимость в
межличностных отношениях, приводящая к социальным / рабочим
проблемам
17.
w/ seasonal patternw/ mood-[congruent, incongruent]
psychotic features
w/ anxious distress
Major depressive disorder
w/ mixed features
w/ peripartum onset
w/ catatonia
w/ atypical features
w/ melancholic features
• delusions &/or hallucinations
• examples of congruent delusions: personal inadequacy, guilt, death, nihilism,
deserved punishment
18.
w/ seasonal patternw/ mood-[congruent, incongruent]
psychotic features
w/ anxious distress
Major depressive disorder
w/ mixed features
w/ peripartum onset
w/ catatonia
w/ atypical features
w/ melancholic features
На протяжении большей части эпизода, ≥3 из следующих:
• stupor
• catalepsy (passive induction of a posture
held against gravity)
• waxy flexibility
• mutism
• negativism
• posturing (spontaneous, maintenance
against gravity)
• mannerism (odd cariacture of a
normal action)
• stereotypy
• agitation (indep of external stimulus)
• grimacing
• echolalia or echopraxia
19.
w/ seasonal patternw/ mood-[congruent, incongruent]
psychotic features
w/ anxious distress
Major depressive disorder
w/ mixed features
w/ peripartum onset
w/ catatonia
w/ atypical features
w/ melancholic features
• во время беременности и (или) 4 недели после родов
20.
w/ seasonal patternw/ mood-[congruent, incongruent]
psychotic features
w/ anxious distress
Major depressive disorder
w/ mixed features
w/ peripartum onset
w/ catatonia
w/ atypical features
w/ melancholic features
• Рецидивы и ремиссии случаются в характерное время года
• Как минимум 2 сезонных MDE за последние 2 года (и никаких несезонных
MDE в течение этого периода)
• На протяжении жизни количество сезонных эпизодов превышает количество
несезонных эпизодов
Если пациент всегда впадает в депрессию из-за сезонной безработицы (или начал
учебного года), назвали бы мы это «сезонным паттерном»? Нет.
21.
The monoamine hypothesis (1965)iproniazid (1957)
imipramine (1959)
Joseph Schildkraut
Belmaker RH and Agam G, NEJM 2008, 358:55-68
22.
chemical inbalanceQuestion:
Имеют ли антидепрессанты дополнительные действия помимо ингибирования
переносчиков обратного захвата?
23.
Chronic antidepressant treatment increases neurogenesis in adult rathippocampus.
Malberg JE, Eisch AJ, Nestler EJ, Duman RS.
J Neurosci. 2000 Dec 15;20(24):9104-10
Requirement of hippocampal neurogenesis for the behavioral effects of
antidepressants.
Santarelli L, Saxe M, Gross C, Surget A, Battaglia F, Dulawa S,
Weisstaub N, Lee J, Duman R, Arancio O, Belzung C, Hen R.
Science. 2003 Aug 8;301(5634):805-9.
Depression and antidepressants: insights from knockout of dopamine,
serotonin or noradrenaline re-uptake transporters.
Haenisch B, Bönisch H.
Pharmacol Ther. 2011 Mar;129(3):352-68. Epub 2010 Dec 13. Review.
Nicotinic acetylcholine receptor antagonistic activity of monoamine
uptake blockers in rat hippocampal slices.
Hennings EC, Kiss JP, De Oliveira K, Toth PT, Vizi ES.
J Neurochem. 1999 Sep;73(3):1043-50.
Block of an ether-a-go-go-like K(+) channel by imipramine rescues egl-2
excitation defects in Caenorhabditis elegans.
Weinshenker D, Wei A, Salkoff L, Thomas JH.
J Neurosci. 1999 Nov 15;19(22):9831-40.
24.
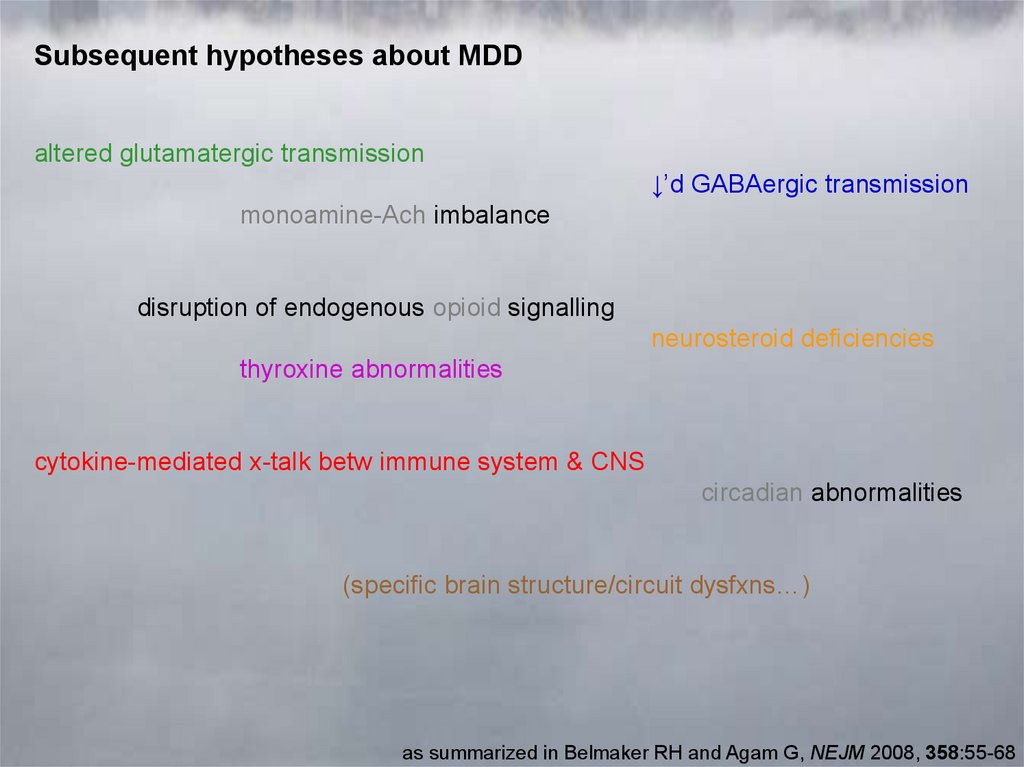
Subsequent hypotheses about MDDaltered glutamatergic transmission
↓’d GABAergic transmission
monoamine-Ach imbalance
disruption of endogenous opioid signalling
neurosteroid deficiencies
thyroxine abnormalities
cytokine-mediated x-talk betw immune system & CNS
circadian abnormalities
(specific brain structure/circuit dysfxns…)
as summarized in Belmaker RH and Agam G, NEJM 2008, 358:55-68
25.
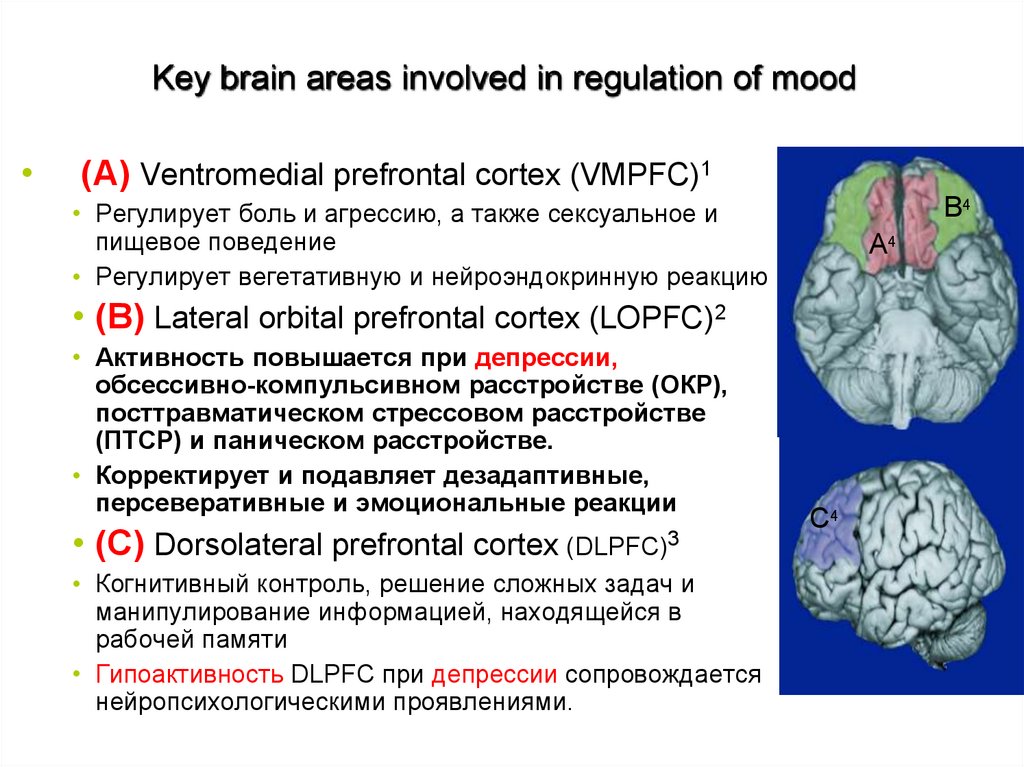
Key brain areas involved in regulation of mood(A) Ventromedial prefrontal cortex (VMPFC)1
B4
• Регулирует боль и агрессию, а также сексуальное и
пищевое поведение
• Регулирует вегетативную и нейроэндокринную реакцию
A4
• (B) Lateral orbital prefrontal cortex (LOPFC)2
• Активность повышается при депрессии,
обсессивно-компульсивном расстройстве (ОКР),
посттравматическом стрессовом расстройстве
(ПТСР) и паническом расстройстве.
• Корректирует и подавляет дезадаптивные,
персеверативные и эмоциональные реакции
• (C) Dorsolateral prefrontal cortex (DLPFC)3
• Когнитивный контроль, решение сложных задач и
манипулирование информацией, находящейся в
рабочей памяти
• Гипоактивность DLPFC при депрессии сопровождается
нейропсихологическими проявлениями. of depression
C4
26.
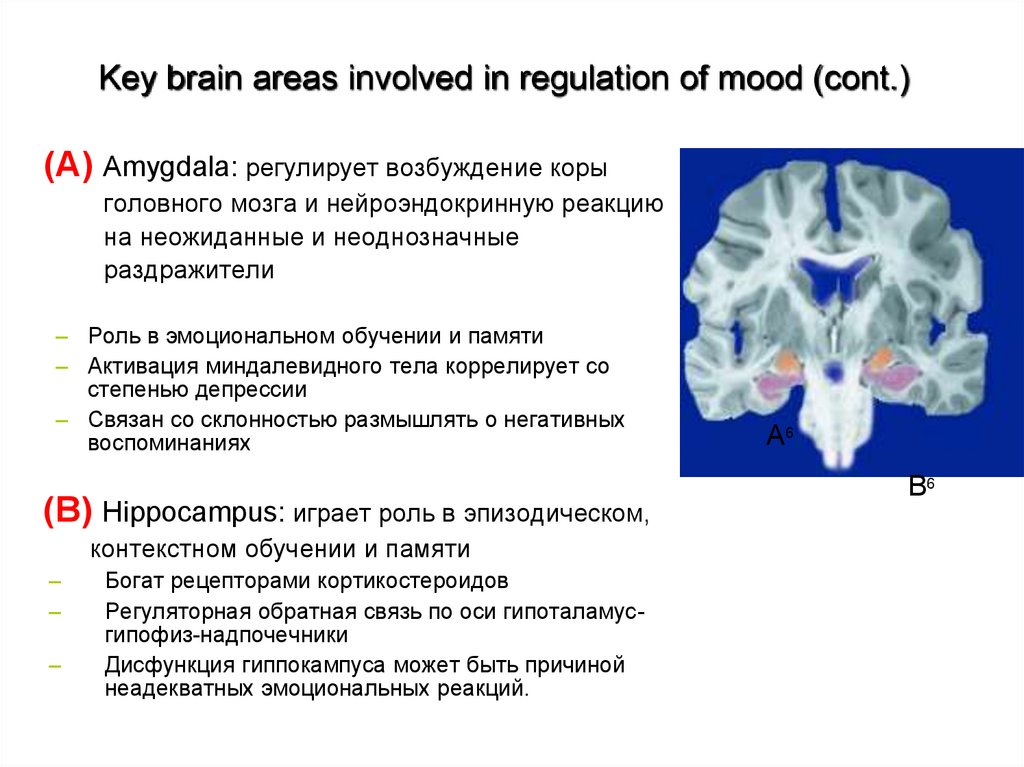
Key brain areas involved in regulation of mood (cont.)(A) Amygdala: регулирует возбуждение коры
головного мозга и нейроэндокринную реакцию
на неожиданные и неоднозначные
раздражители
– Роль в эмоциональном обучении и памяти
– Активация миндалевидного тела коррелирует со
степенью депрессии
– Связан со склонностью размышлять о негативных
воспоминаниях
A6
B6
(B) Hippocampus: играет роль в эпизодическом,
контекстном обучении и памяти
–
–
–
Богат рецепторами кортикостероидов
Регуляторная обратная связь по оси гипоталамусгипофиз-надпочечники
Дисфункция гиппокампуса может быть причиной
неадекватных эмоциональных реакций.
53
27.
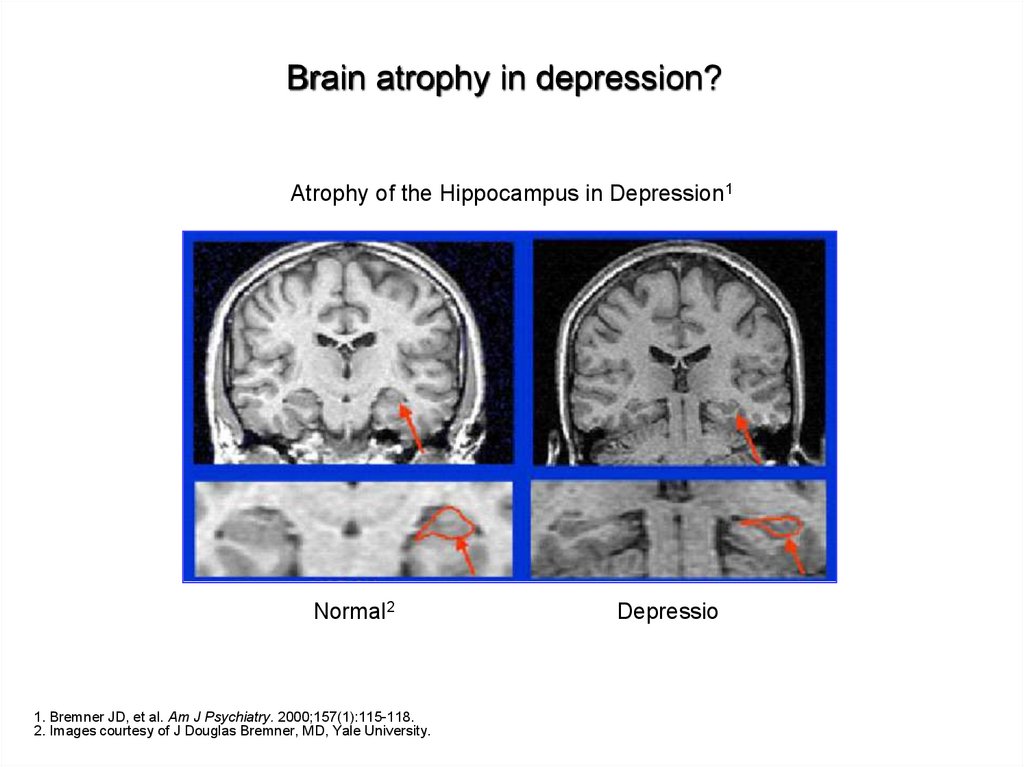
Brain atrophy in depression?Atrophy of the Hippocampus in Depression1
Normal2
1. Bremner JD, et al. Am J Psychiatry. 2000;157(1):115-118.
2. Images courtesy of J Douglas Bremner, MD, Yale University.
Depression2
28.
Major Depression: CognitionПриобретенная (выученная) беспомощность
(Seligman) (Seligman & Maier, 1967)
• Приписывание отсутствия контроля над стрессом приводит к тревоге и
депрессии
• Присущ депрессивный стиль - внутренний, стабильный и глобальный
Отрицательный когнитивные стиль
(A. Beck)
Депрессия является результатом негативных интерпретаций (ношение серых
очков вместо розовых, например, Иа в Винни-Пухе)
Ключевые компоненты отрицательных интерпретаций
Неадаптивное отношение (негативная схема) «Я нехороший» (я), «Другим
нельзя доверять» (другие нехорошие) и «усилия не окупаются »(мир
нехороший)
•Автоматические мысли
•Когнитивная триада
29
•Ошибки в оценке окружающей действительностидействительностиn thinking
29.
Seligman & BeckSeligman
Attributions are:
•Internal
•Stable
•Global
Beck (NegativeTriad)
Negative interpretations about:
•Themselves
•Immediate world
•Future
Я неадекватен (внутренний) во
всем (глобальный) и всегда буду
(стабильный).
«Темные очки о том, почему все
плохо»
Я плохо учусь в школе (Я). Я
ненавижу этот кампус
(окружающий меня мир). Дела в
колледже (в будущем) не пойдут
хорошо.
“Темные очки о том, что
происходит” on”
30
30.
Cognitive theories• Beck’s theory:
Характер пессимизма (Негативная триада)
Привычки к негативу (негативные схемы)
Ошибочное мышление (характерные предубеждения)
DEPRESSION
31
31.
Characteristic biasesНеоднозначные вывод
Селективная абстракция
Чрезмерное обобщение
Преувеличение и преуменьшение
32
32.
Behavioral theoriesПриученная беспомощность / безнадежность - это поведенческая
теория с акцентом на когнитивный элемент.
Уменьшение подкрепления (поддержки) ведет к снижению
активности.
Усиливается депрессивное поведение.
Депрессия have taken part in fewer pleasant events.
34
33.
Interpersonal theoryСнижение межличностной поддержки
Отрицательный опыт неприятия окружающими
Из-за социального несоответствия
Неадекватные социальные связи
Другим они могут не нравиться
Вызвано пациентом
Последствия поведенческого выбора
Критические комментарии супруга
Плохие социальные навыки и в поиске поддержки
33
34.
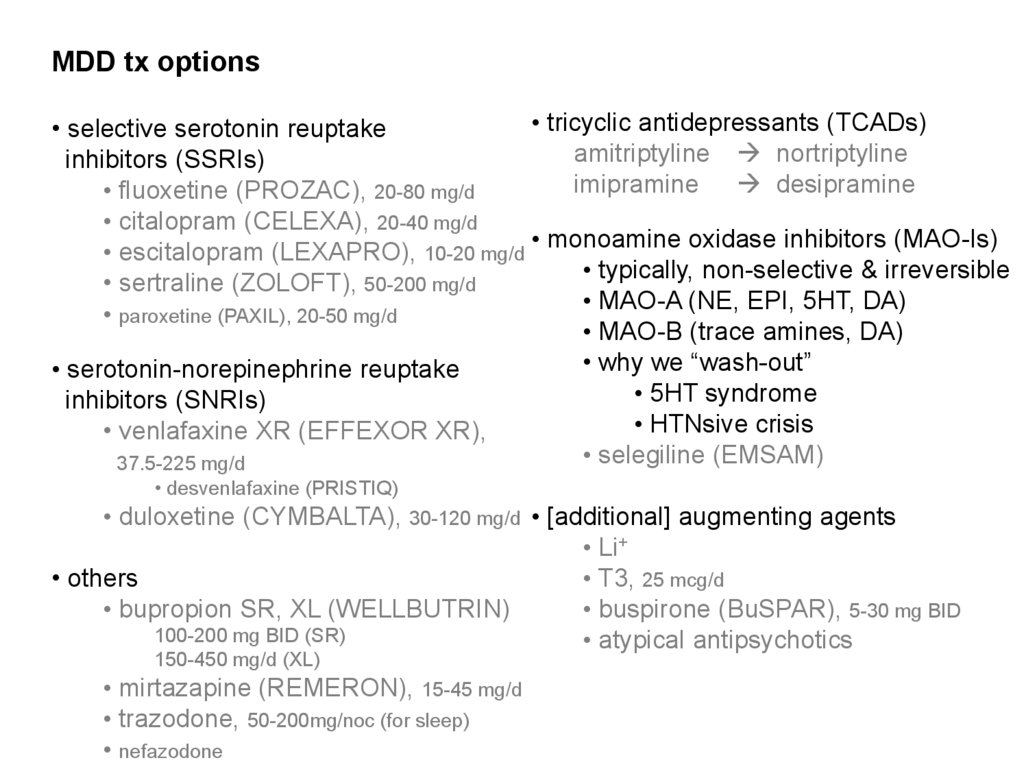
MDD tx options• tricyclic antidepressants (TCADs)
• selective serotonin reuptake
amitriptyline nortriptyline
inhibitors (SSRIs)
imipramine desipramine
• fluoxetine (PROZAC), 20-80 mg/d
• citalopram (CELEXA), 20-40 mg/d
• monoamine oxidase inhibitors (MAO-Is)
• escitalopram (LEXAPRO), 10-20 mg/d
• typically, non-selective & irreversible
• sertraline (ZOLOFT), 50-200 mg/d
• MAO-A (NE, EPI, 5HT, DA)
• paroxetine (PAXIL), 20-50 mg/d
• MAO-B (trace amines, DA)
• why we “wash-out”
• serotonin-norepinephrine reuptake
• 5HT syndrome
inhibitors (SNRIs)
• HTNsive crisis
• venlafaxine XR (EFFEXOR XR),
• selegiline (EMSAM)
37.5-225 mg/d
• desvenlafaxine (PRISTIQ)
• duloxetine (CYMBALTA), 30-120 mg/d • [additional] augmenting agents
• Li+
• others
• T3, 25 mcg/d
• bupropion SR, XL (WELLBUTRIN)
• buspirone (BuSPAR), 5-30 mg BID
100-200 mg BID (SR)
• atypical antipsychotics
150-450 mg/d (XL)
• mirtazapine (REMERON), 15-45 mg/d
• trazodone, 50-200mg/noc (for sleep)
• nefazodone
35.
MDD tx options• Ψtherapy
• cognitive bx therapy (CBT)
• interpersonal therapy (IPT)
• psychodynamic therapy
• interventional Ψ
• electroconvulsive therapy (ECT)
• transcranial magnetic stimulation (TMS)
• vagal nerve stimulation (VNS)
• deep brain stimulation (DBS)
• 80-90% remission rate
• 50-80% relapse rate (6mos out)
• SEs: musculoskeletal, headache,
cognitive
• mania, catatonia, NMS (other
indixn’s)
• other
• lightbox therapy (mostly for MDD w/ seasonal features)
Devanand DP et al, 1991
36.
Major Depressive D/O (MDD)NATURAL HISTORY (Frank E and Thase ME, 1999 & DSM-5)
• recovery usually begins:
• w/in 3mos for two in five indivs
• w/in 1y for four in five indivs
• risk of subsequent episodes (w/in 3y) increases w/ n:
• ≥50% if n=1
• ≥70% if n=2
• ≥90% if n=3
• dz course does not typically change as one ages
• 5-10% will eventually be dx’d w/ bipolar disorder (BD)
• more likely w/:
• onset of ‘MDD’ in adolescence
• a family history of BD
• ‘mixed features’
• 6% lifetime SUI risk; up to 15% w/ severe MDD
37.
Progression of depression — “kindling” phenomenon: Adverseeffects of each successive episode
10
Likelihood of recent life stress precipitating depression
Risk (OR) of depression onset per month
Female subjects only N=2395
Risk (Odds Ratio)
8
6
4
2
0
0
1
2
3
4
5
6
7-8
Number of Previous Depressive Episodes
Kendler KS, et al. Am J Psychiatry. 2000;157(8):1243-1251.
11
9-11
38.
Persistent depressive disorder (dysthymia)• 2y подавленного настроения (1 год у детей / подростков) большую часть дня,
больше дней есть, чем нет, плюс 2 из следующих :
• appetite disturbance (↓ or ↑)
• sleep disturbance (↓ or ↑)
• ↓energy
• ↓esteem
• poor [ ]
• hopeless
• never sx-free for more than 2mos at a time
• overlapping dx of MDD is now allowed
• there has never been mania, hypomania, or cyclothymia
• MDD specifiers can also be used for dysthymia
• additionally:
• early onset (before age 21)
• w/ persistent MDE
• late onset (at age 21 or older) • w/ intermittent MDE’s, w/ current episode
• w/ pure dysthymic syndrome • w/ intermittent MDE’s, w/o current episode
--
from DSM-5
39.
Persistent depressive disorder (dysthymia)•может быть более устойчивым к лечению (TxR), чем MDD
ЭПИДЕМИОЛОГИЯ
• Распространенность на протяжение жизни = 6%
• Распространенность через 12 месяцев = 0,5%, по сравнению с 1,5% для БДР
• Высокая ко-морбидность с расстройствами личности (особенно кластеры B, C)
From Sadock & Sadock & DSM-5
40.
Premenstrual dysphoric d/oКритерий А. В большинстве менструальных циклов ≥5 симптомов за последнюю
неделю перед началом менструации, с улучшением через несколько дней
после ее начла и практически отсутствует в течение недели в
постменструальную фазу
Критерий Б. ≥1 (или более) симптомов:
1. лабильность (например, перепады настроения, внезапная грусть, повышенная
чувствительность к невниманию окружающих)
2. раздражительность / гнев / увеличение межличностных конфликтов
3. тревога / напряжение / возбужденное состояние / нервозность
41.
Premenstrual dysphoric d/oКритерий C. ≥1 (или более) sx для достижения в сумме 5 очков в схватке с
предыдущим списком:
1. Ангедония
2. Нарушение концентрации
3. Анергия
4. Значительное изменение аппетита (включая особую тягу к еде)
5. Нарушение сна (↑ или ↓)
6. Чувство подавленности или неконтролируемости
7. Соматические симптомы (болезненность / припухлость груди,
артралгии/миалгии, вздутие живота, увеличение массы тела)
Особые примечания. Это не может быть просто обострение менструального
цикла при MDD или других психиатрических расстройств;
должно иметь подтверждение предполагаемыми ежедневными рейтинговыми
шкалами в течение не менее 2-х циклов
42.
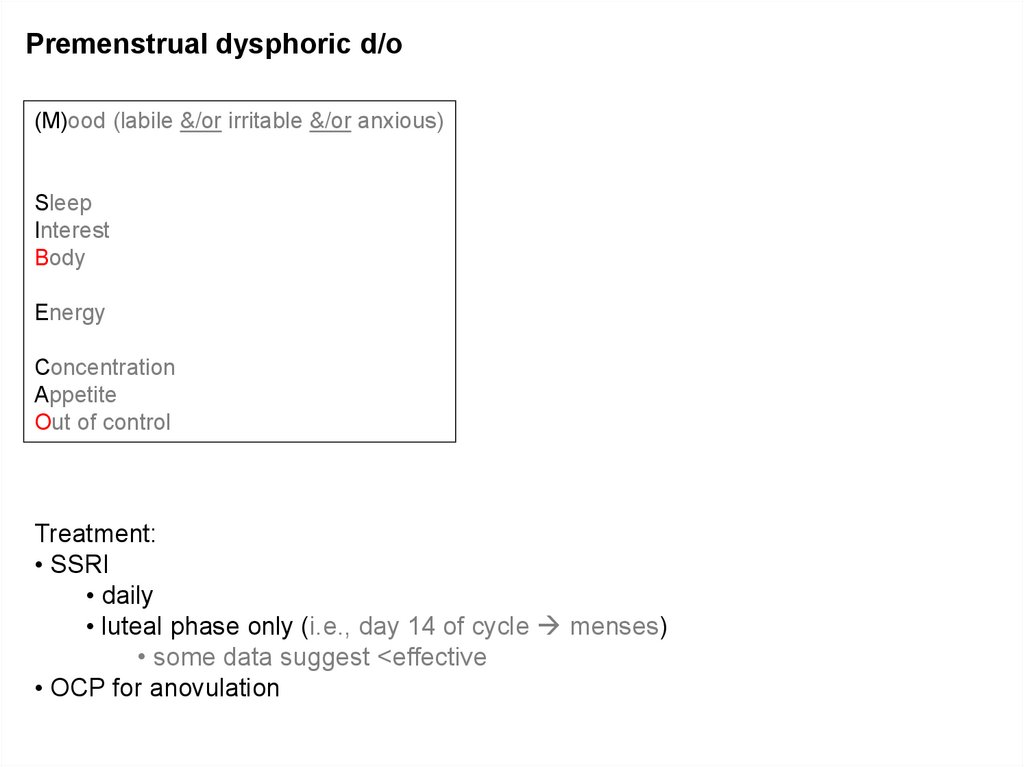
Premenstrual dysphoric d/o(M)ood (labile &/or irritable &/or anxious)
Sleep
Interest
Body
Energy
Concentration
Appetite
Out of control
Treatment:
• SSRI
• daily
• luteal phase only (i.e., day 14 of cycle menses)
• some data suggest <effective
• OCP for anovulation
43.
Bipolar disorder44.
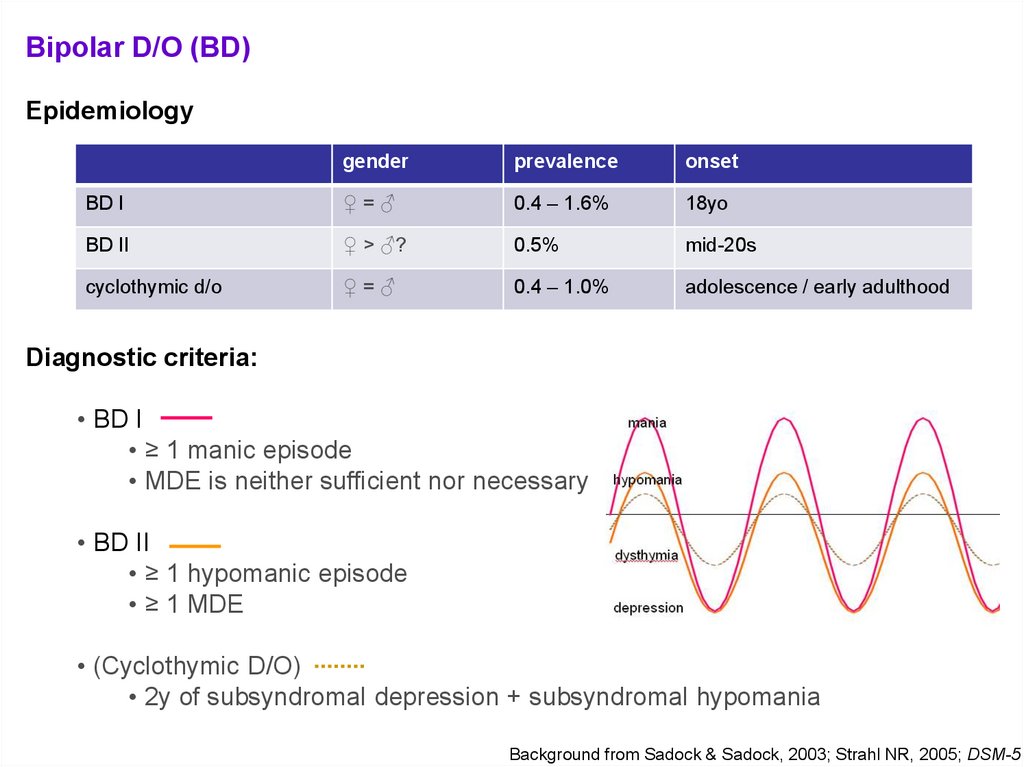
Bipolar D/O (BD)Epidemiology
gender
prevalence
onset
BD I
♀=♂
0.4 – 1.6%
18yo
BD II
♀ > ♂?
0.5%
mid-20s
cyclothymic d/o
♀=♂
0.4 – 1.0%
adolescence / early adulthood
Diagnostic criteria:
• BD I
• ≥ 1 manic episode
• MDE is neither sufficient nor necessary
• BD II
• ≥ 1 hypomanic episode
• ≥ 1 MDE
• (Cyclothymic D/O)
• 2y of subsyndromal depression + subsyndromal hypomania
Background from Sadock & Sadock, 2003; Strahl NR, 2005; DSM-5
45.
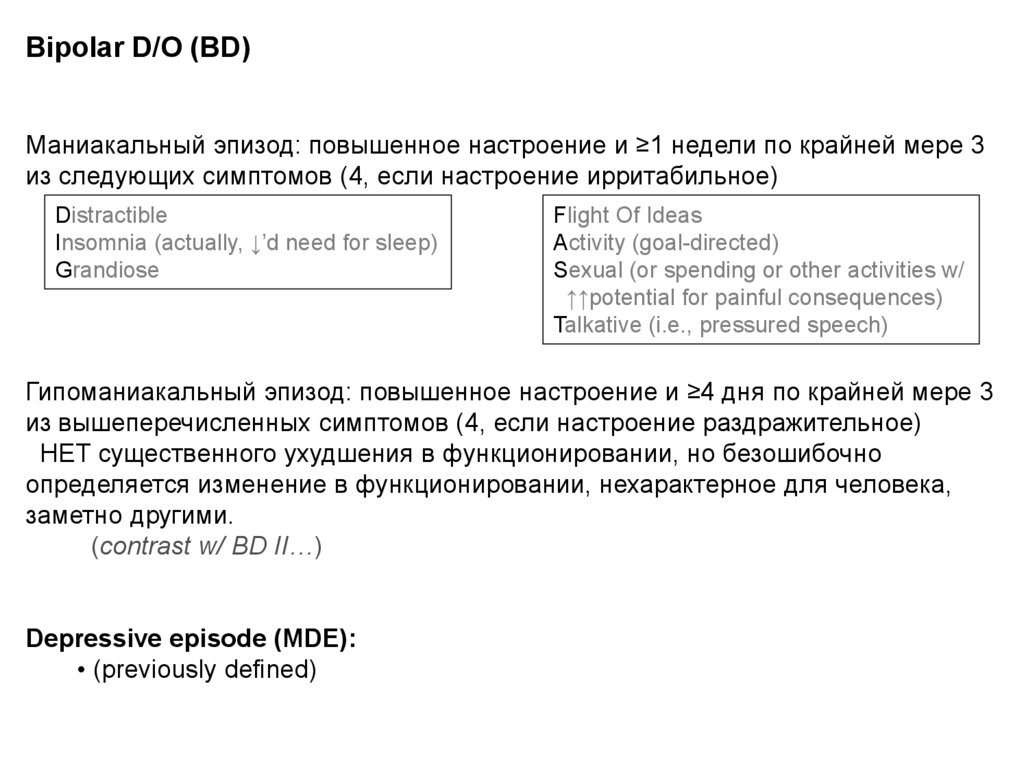
Bipolar D/O (BD)Маниакальный эпизод: повышенное настроение и ≥1 недели по крайней мере 3
из следующих симптомов (4, если настроение ирритабильное)
Distractible
Insomnia (actually, ↓’d need for sleep)
Grandiose
Flight Of Ideas
Activity (goal-directed)
Sexual (or spending or other activities w/
↑↑potential for painful consequences)
Talkative (i.e., pressured speech)
Гипоманиакальный эпизод: повышенное настроение и ≥4 дня по крайней мере 3
из вышеперечисленных симптомов (4, если настроение раздражительное)
НЕТ существенного ухудшения в функционировании, но безошибочно
определяется изменение в функционировании, нехарактерное для человека,
заметно другими.
(contrast w/ BD II…)
Depressive episode (MDE):
• (previously defined)
46.
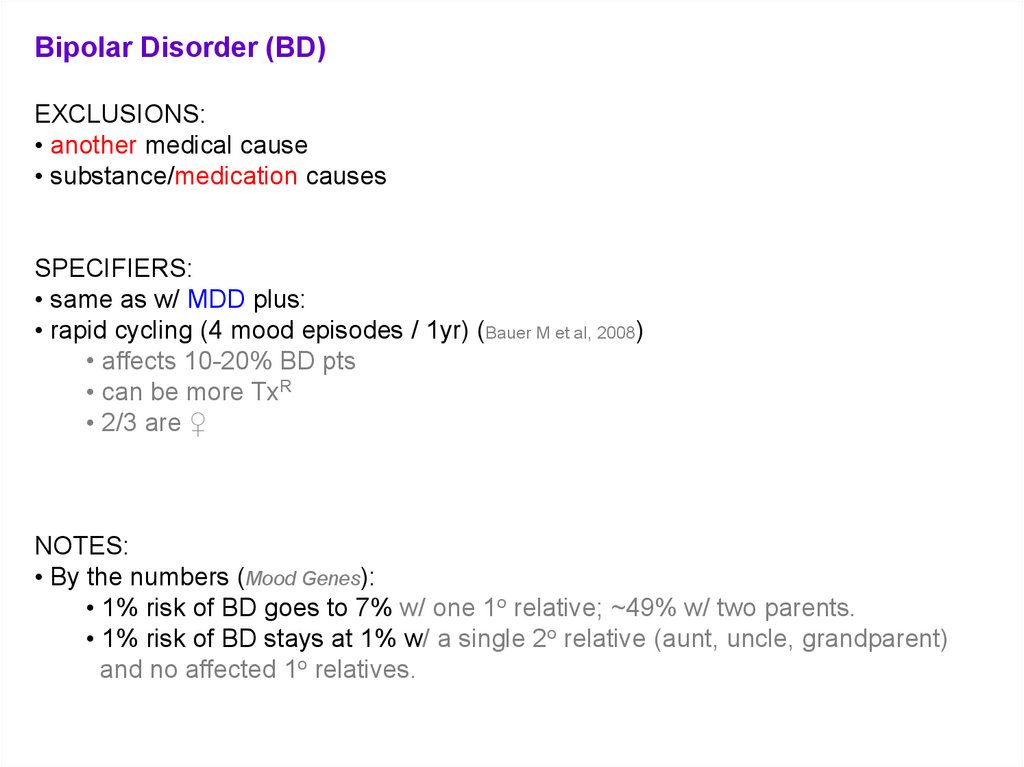
Bipolar Disorder (BD)EXCLUSIONS:
• another medical cause
• substance/medication causes
SPECIFIERS:
• same as w/ MDD plus:
• rapid cycling (4 mood episodes / 1yr) (Bauer M et al, 2008)
• affects 10-20% BD pts
• can be more TxR
• 2/3 are ♀
NOTES:
• By the numbers (Mood Genes):
• 1% risk of BD goes to 7% w/ one 1o relative; ~49% w/ two parents.
• 1% risk of BD stays at 1% w/ a single 2o relative (aunt, uncle, grandparent)
and no affected 1o relatives.
47.
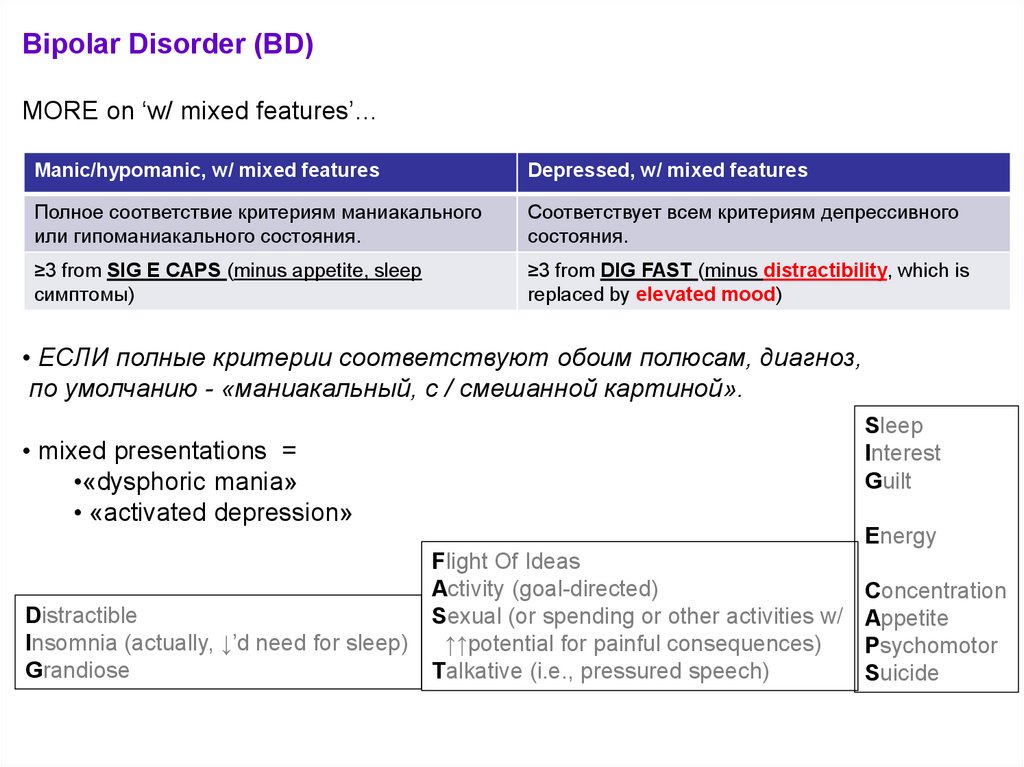
Bipolar Disorder (BD)MORE on ‘w/ mixed features’…
Manic/hypomanic, w/ mixed features
Depressed, w/ mixed features
Полное соответствие критериям маниакального
или гипоманиакального состояния.
Соответствует всем критериям депрессивного
состояния.
≥3 from SIG E CAPS (minus appetite, sleep
симптомы)
≥3 from DIG FAST (minus distractibility, which is
replaced by elevated mood)
• ЕСЛИ полные критерии соответствуют обоим полюсам, диагноз,
по умолчанию - «маниакальный, с / смешанной картиной».
Sleep
Interest
Guilt
• mixed presentations =
•«dysphoric mania»
• «activated depression»
Energy
Distractible
Insomnia (actually, ↓’d need for sleep)
Grandiose
Flight Of Ideas
Activity (goal-directed)
Sexual (or spending or other activities w/
↑↑potential for painful consequences)
Talkative (i.e., pressured speech)
Concentration
Appetite
Psychomotor
Suicide
48.
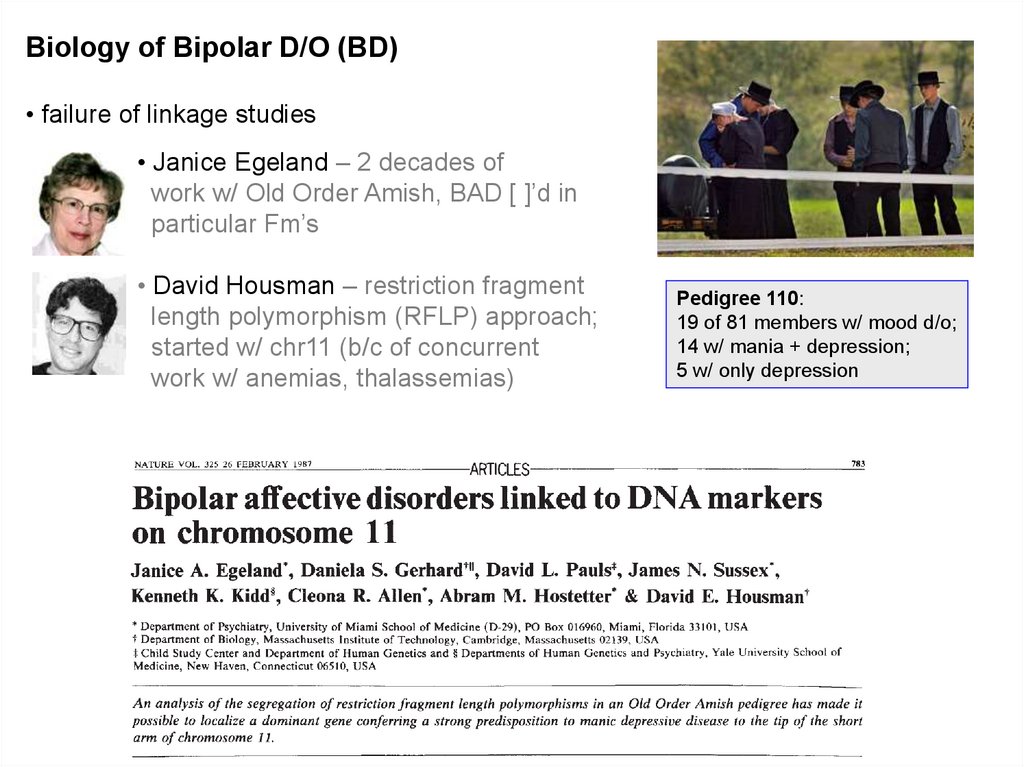
Biology of Bipolar D/O (BD)• failure of linkage studies
• Janice Egeland – 2 decades of
work w/ Old Order Amish, BAD [ ]’d in
particular Fm’s
• David Housman – restriction fragment
length polymorphism (RFLP) approach;
started w/ chr11 (b/c of concurrent
work w/ anemias, thalassemias)
Pedigree 110:
19 of 81 members w/ mood d/o;
14 w/ mania + depression;
5 w/ only depression
49.
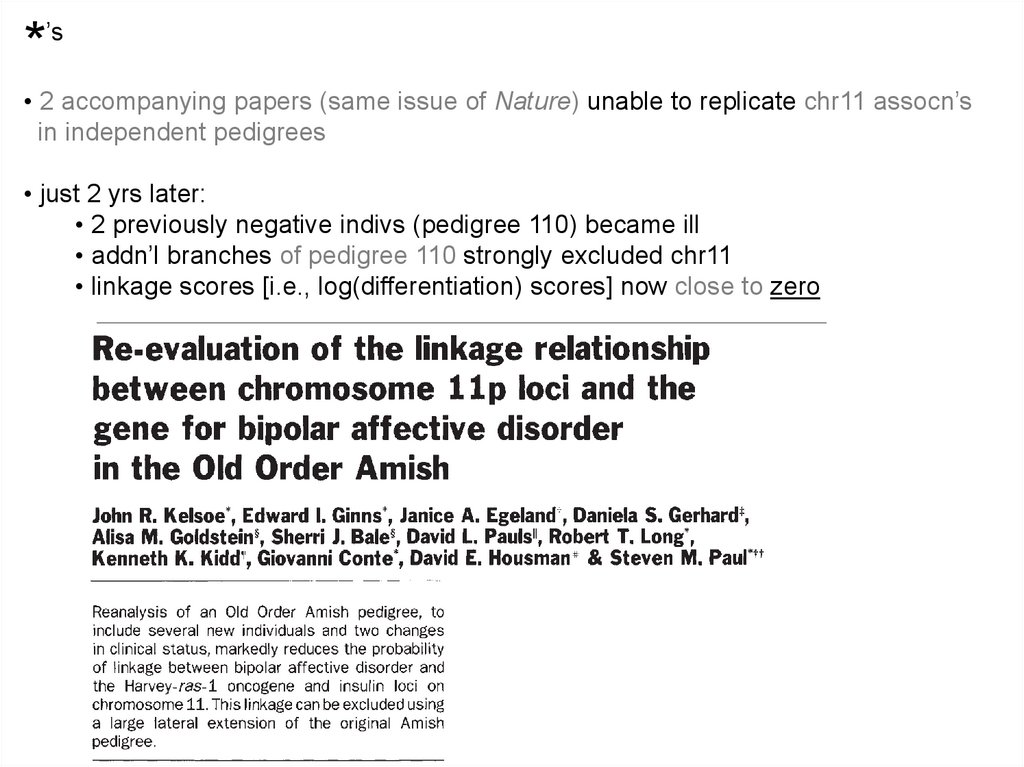
*’s
• 2 accompanying papers (same issue of Nature) unable to replicate chr11 assocn’s
in independent pedigrees
• just 2 yrs later:
• 2 previously negative indivs (pedigree 110) became ill
• addn’l branches of pedigree 110 strongly excluded chr11
• linkage scores [i.e., log(differentiation) scores] now close to zero
50.
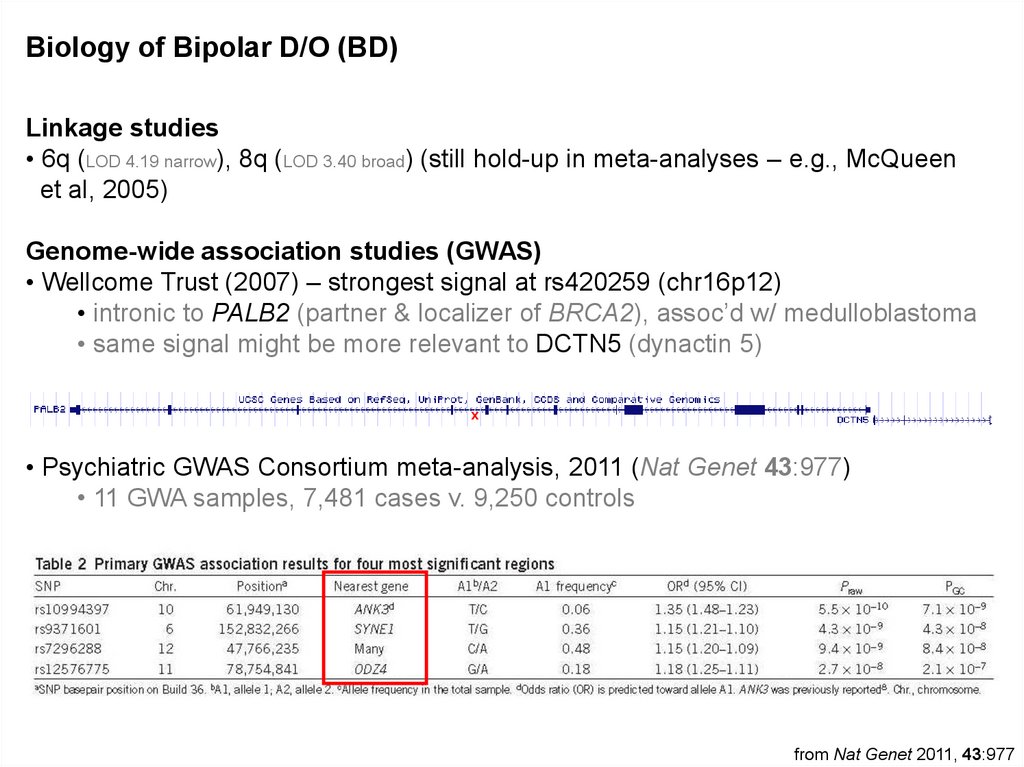
Biology of Bipolar D/O (BD)Linkage studies
• 6q (LOD 4.19 narrow), 8q (LOD 3.40 broad) (still hold-up in meta-analyses – e.g., McQueen
et al, 2005)
Genome-wide association studies (GWAS)
• Wellcome Trust (2007) – strongest signal at rs420259 (chr16p12)
• intronic to PALB2 (partner & localizer of BRCA2), assoc’d w/ medulloblastoma
• same signal might be more relevant to DCTN5 (dynactin 5)
x
• Psychiatric GWAS Consortium meta-analysis, 2011 (Nat Genet 43:977)
• 11 GWA samples, 7,481 cases v. 9,250 controls
from Nat Genet 2011, 43:977
51.
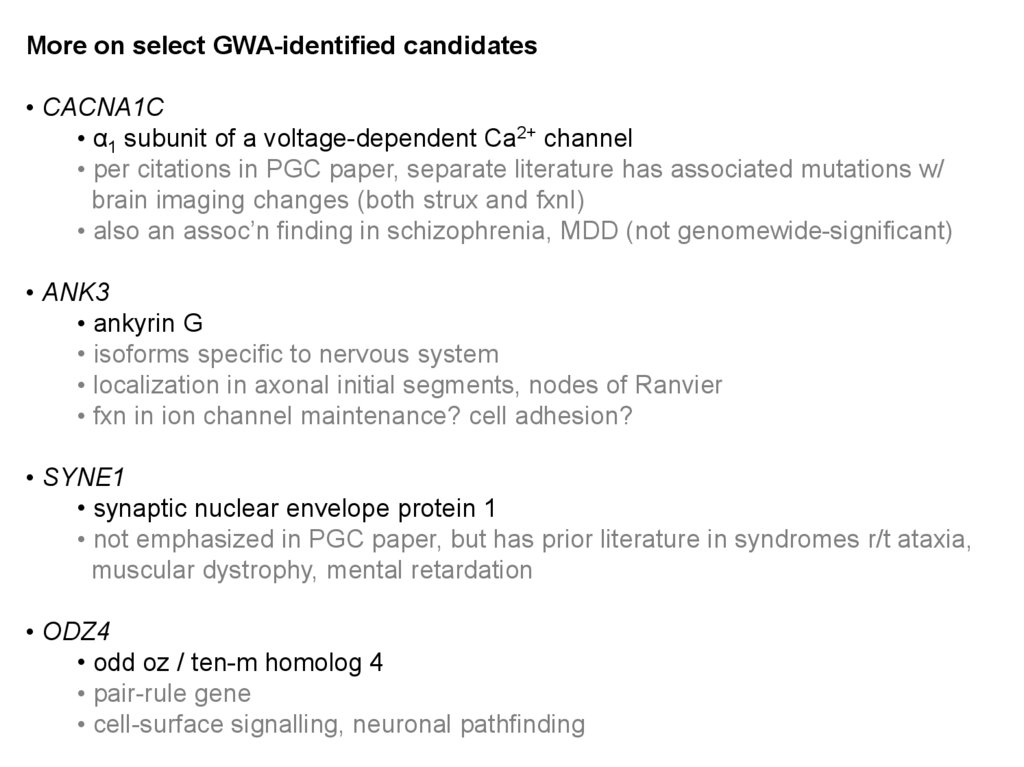
More on select GWA-identified candidates• CACNA1C
• α1 subunit of a voltage-dependent Ca2+ channel
• per citations in PGC paper, separate literature has associated mutations w/
brain imaging changes (both strux and fxnl)
• also an assoc’n finding in schizophrenia, MDD (not genomewide-significant)
• ANK3
• ankyrin G
• isoforms specific to nervous system
• localization in axonal initial segments, nodes of Ranvier
• fxn in ion channel maintenance? cell adhesion?
• SYNE1
• synaptic nuclear envelope protein 1
• not emphasized in PGC paper, but has prior literature in syndromes r/t ataxia,
muscular dystrophy, mental retardation
• ODZ4
• odd oz / ten-m homolog 4
• pair-rule gene
• cell-surface signalling, neuronal pathfinding
52.
Bipolar Disorder (BD) – treatmentThe old standard:
• mood stabilizer + reuptake blocker
FDA-approved Rxs for BD
Debunked:
• gabapentin (NEURONTIN)
• topirimate (TOPAMAX)
53.
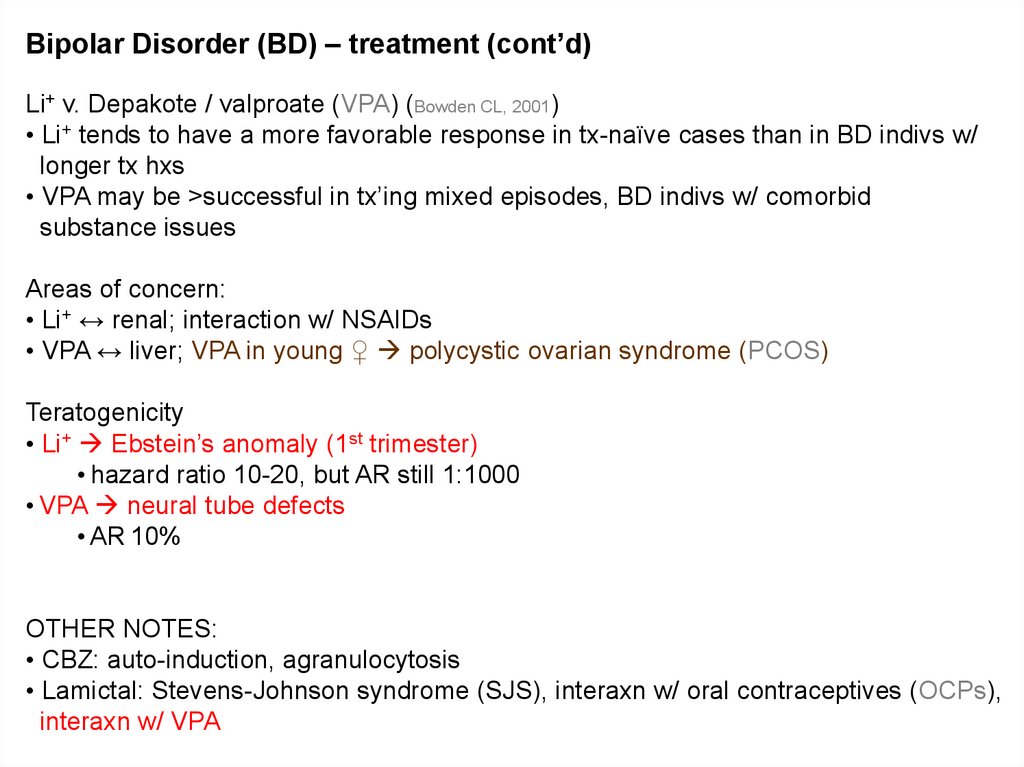
Bipolar Disorder (BD) – treatment (cont’d)Li+ v. Depakote / valproate (VPA) (Bowden CL, 2001)
• Li+ tends to have a more favorable response in tx-naïve cases than in BD indivs w/
longer tx hxs
• VPA may be >successful in tx’ing mixed episodes, BD indivs w/ comorbid
substance issues
Areas of concern:
• Li+ ↔ renal; interaction w/ NSAIDs
• VPA ↔ liver; VPA in young ♀ polycystic ovarian syndrome (PCOS)
Teratogenicity
• Li+ Ebstein’s anomaly (1st trimester)
• hazard ratio 10-20, but AR still 1:1000
• VPA neural tube defects
• AR 10%
OTHER NOTES:
• CBZ: auto-induction, agranulocytosis
• Lamictal: Stevens-Johnson syndrome (SJS), interaxn w/ oral contraceptives (OCPs),
interaxn w/ VPA
54.
Bipolar Disorder (BD) – treatment (cont’d)How many agents to use?
• combination tx often helpful in acute stabilization
• antipsychotics REQ’D when there are psychotic features to mood episode
Adjuncts
• benzos
--Don’t forget about ECT…
Manic switch w/…
• reuptake blockers
• Lamictal, too! (van der Loos ML et al, 2009)
55.
Bipolar Disorder (BD) – natural history• 60% маниакальных эпизодов перейдут, практически сразу, в MDE
• MDE обычно значительно превышает количество гипоманиакальных и
маниакальных эпизодов.
• ~ 10% от BD II BD I
• эпизоды имеют тенденцию увеличиваться по частоте / продолжительности с
возрастом
• re: самоубийство ...
• 35% -ная распространенность хотя бы одной SUI попытки в течение жизни у
биполярных пациентов
• 15% самоубийств (может быть немного завышенной оценкой)
• В 15 раз выше риск по сравнению с населения в целом (для завершенных)
• возможно, ¼ всех самоубийств среди населения
• > летальность попыток SUI у BD II выше, чем (чем BD I)
adapated, in part,from DSM-5
56.
Cyclothymic D/O•2 года переменчивого настроения (1 год у детей, подростков)
• гипоманиакальные симптомы (но НЕ эпизоды)
• дистимические симптомы (но без MDE)
• ≥ в в течение 2 х лет не менее года, в общей сложности и (не более 2
мес за это время полное отсутствие симптомов)
ИСКЛЮЧЕНИЯ
• нет маниакальных / гипоманиакальных эпизодов
• нет депрессивных эпизодов
57.
Differential diagnosis58.
Phenocopies and gray areas…• Anxiety D/O’s (esp. GAD, PTSD)
• Schizoaffective D/O
• Delirium
• Dementia
• Personality D/O’s
• Substance/Medication-induced Depressive D/O
• Depressive D/O d/t Another Medical Condition
• Other Specified Depressive D/O
• Unspecified Depressive D/O
• Substance/Medication-induced Bipolar and Related D/O
• Bipolar and Related D/O d/t Another Medical Condition
• Other Specified Bipolar and Related D/O
• Unspecified Bipolar and Related D/O
59.
Depressive, Bipolar & Related D/O d/t a Another Medical Condition• Endocrine (e.g., thyroid, hypothalamic-pituitary-adrenal/HPA)
• Neurologic (e.g., multiple sclerosis, CVA, brain tumor, Parkinson’s, Alzheimer’s/other
dementia, Huntington’s, seizure d/o)
• Neoplastic (e.g., pancreas)
• TBI
• Autoimmune (e.g., neuropsychiatric systemic lupus erythematosus / NPSLE)
• Hematologic (e.g., acute intermittent porphyria / AIP)
• typically: anx/depr >> s/t Ψosis, mania (rare)
• acute abdominal pain, muscle weakness
• port wine-colored urine (porphobilinogen)
• transient damage to nerve cells
• Nutritional (e.g., B12)
• Infectious (e.g., HIV, Syphilis)
60.
Substance/Medication-induced Depressive, Bipolar & Related D/OILLICITS
• can be from intoxication or withdrawal phases
• EtOH – typically depressive
• stimulants – typically manic/hypomanic
• --good to ask about sxs during windows of sobriety (ideally, ≥6mos)
• high substance comorbidity rates w/ endogenous Axis I Ψ d/o’s, though (esp. BD I)
Prescription Rxs
• steroids
• IFN-α2b, RBV (HCV tx)
• β-blockers
• antidepressants
• α-TB drugs
61.
Mood D/O’s lab w/u• CBC
• Chem panel
• TSH
• B12
• U-tox
• U-preg (dep on demographics)
• RPR (syphilis)
• HIV-1,2 ELISA (lower threshold for BD patients…)
62.
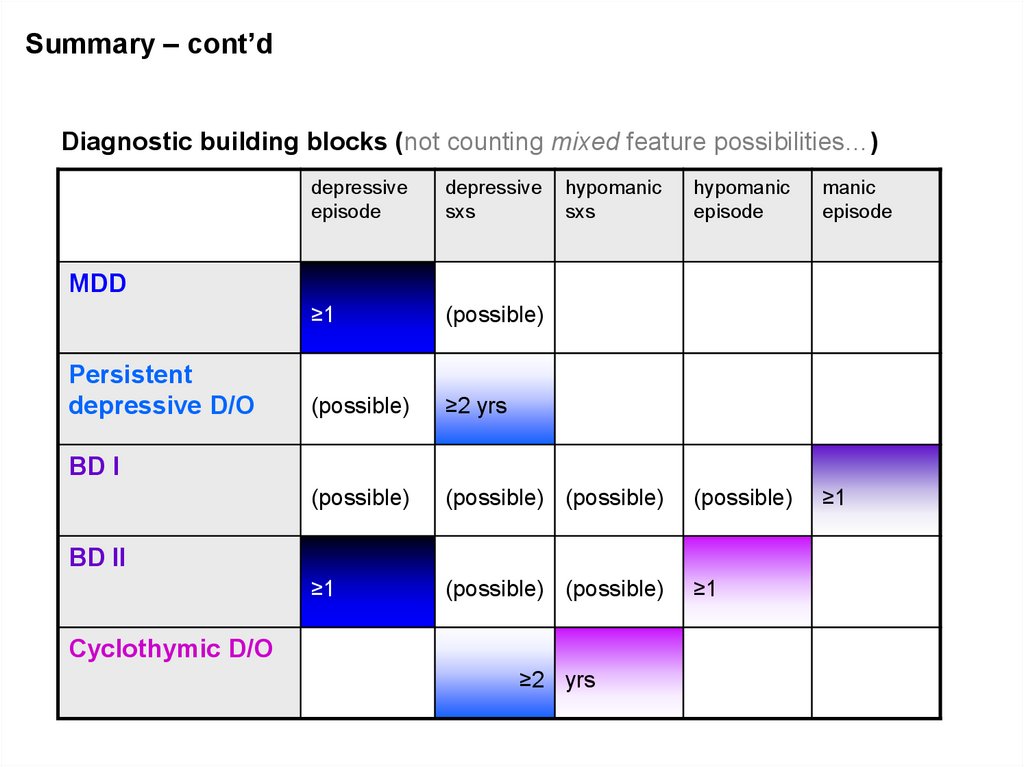
Summary – cont’dDiagnostic building blocks (not counting mixed feature possibilities…)
depressive
episode
depressive
sxs
hypomanic
sxs
hypomanic
episode
manic
episode
≥1
(possible)
(possible)
≥2 yrs
(possible)
(possible) (possible)
(possible)
≥1
≥1
(possible) (possible)
≥1
MDD
Persistent
depressive D/O
BD I
BD II
Cyclothymic D/O
≥2 yrs
63.
5 Myths and Facts About SuicideMyth #1:
Fact:
• People who talk
•Most people who
about killing
commit suicide
themselves rarely have given some
commit suicide.
verbal clues or
warnings of their
intentions
40
64.
5 Myths and Facts About SuicideMyth #2:
• The suicidal person
wants to die and feels
there is no turning back.
Fact:
•Suicidal people are
usually ambivalent
about dying; they may
desperately want to live
but can not see
alternatives to
problems.
41
65.
5 Myths and Facts About SuicideMyth # 3:
• If you ask someone
about their suicidal
intentions, you will only
encourage them to kill
themselves.
Fact:
•The opposite is true.
Asking lowers their
anxiety and helps deter
suicidal behavior.
Discussion of suicidal
feelings allow for
accurate risk
assessment.
42
66.
5 Myths and Facts About SuicideMyth # 4:
• All suicidal people are
deeply depressed.
Fact:
•Although suicide is
usually associated with
depression, not all
suicidal people are
obviously depressed.
Once they make the
decision, they may
appear
happier/carefree.
43
67.
5 Myths and Facts About SuicideMyths # 5:
• Suicidal people rarely
seek medical attention.
Fact:
•75% of suicidal
individuals will visit a
physician within the
month before they kill
themselves.
44
68.
Socio-demographic Risk FactorsMale
> 60 years
Widowed or Divorced
White or Native American
Living alone (social isolation)
Unemployed (financial difficulties)
Recent adverse life events
Chronic Illness
45
69.
Clinical Risk FactorsPrevious Attempts
Clinical depression or schizophrenia
Substance Abuse
Feelings of hopelessness
Severe anxiety, particularly with depression
Severe loss of interest in usual activities
Impaired thought process
Impulsivity
46
70.
Suicide:TreatmentProblem-solving
Cognitive behavioral therapy
Coping skills
Stress reduction
47
71.
72.
Major depressive disorder (MDD) – Key PointsMDD может быть хроническим, рецидивирующим и
прогрессирующим заболеванием.
MDD связано с функциональными и структурными
изменениями в головном мозге.
MDD, стресс и боль связаны со схожей супрессией
нейротрофических факторов и нарушением
нейропластичности.
Ремиссия, а не ответ на антидепрессант конечная цель лечения
73.
• Расстройство настроения - это психической состояния, при которомэмоциональная дисрегуляция является основной проблемой.
Падение настроения может быть эндогенным, из-за веществ / лекарств или
из-за другого расстройства здоровья.
• Есть дополнительные фенокопии, которые всегда должны быть в диф.
диагнозе, включая тревожные расстройства, Schizoaffective, Personality
Disorder, Delirium, и различные нейрокогнитивные нарушения.
Чуть меньше ½ пациентов, не получавших ранее лечения, ответят на свой
первый антидепрессант; только 1/3 выздоровеет без лечения.
Немедикаментозные подходы к лечению депрессивных расстройств
включают и не медикаментозную терапию - психотерапию идругие
интервенционные процедуры (например, ЭСТ).
74.
``qw0110