




 are formed from the fibrous connective tissue and are divided into the following")


















 Биология
БиологияПохожие презентации:










Articular system
1. ARTICULAR SYSTEM
GENERALINFORMATION
2. PLAN:
1.2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
Development of joints.
Classification of bone articulations.
Continuous bone articulations.
Synovial joints.
The most typical features of the joints.
Accessory structures of joints.
Congruent and incongruent joints.
Movements in the joints.
Classification of the joints based on the number of articulating
surfaces.
Classification of the joints based on the shape of articulating surfaces.
Clinical applications.
3. Development of joints
Embryonic development of the joints is greatlydependent on the bone development. In the areas, where
discontinuous articulations will form between the developing
bones, the mesenchyme is resorbed in the center of the
primordium forming a cleft-like cavity of the future joint. On
the contrary, peripheral regions of the mesenchyme, which
surround the cavity, condense, giving rise to the fibrous
capsule and ligaments of the joint. Cartilaginous epiphyses
ossify in such away that a thin layer of articular cartilage
remains on their surfaces for life, which provides the
smoothness of articular surfaces.
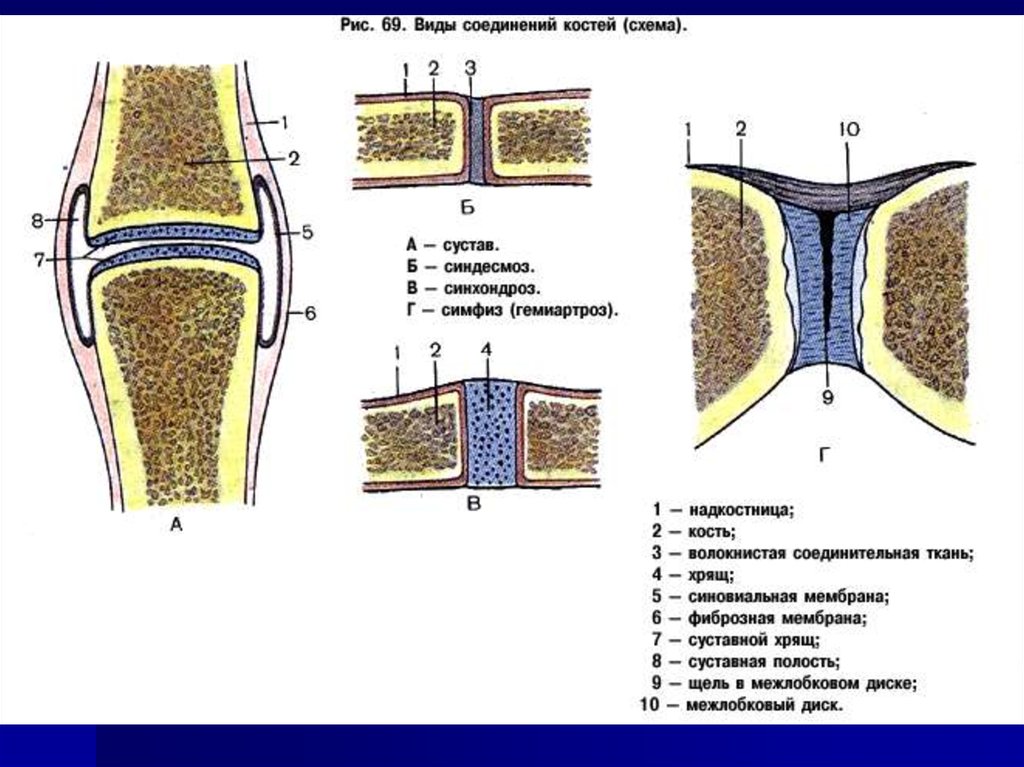
4. CLASSIFICATION OF BONE ARTICULATIONS
Continuous articulations(synarthroses) are characterized bythe presence of an uninterrupted articulating tissue -connective,
cartilaginous, or osseous. Such articulations are either slightly
movable or completely fixed.
Discontinuous (synovial) articulations contain a cavity lined
with the synovial membrane. They possess a great mobility. They
are called joints.
Intermediate forms between the continuous and discontinuous
articulations are symphyses (or hemiarthroses). They are
represented by the cartilaginous articulations with the cleft-like
cavity lacking a fibrous capsule and without synovial membrane.
5. CONTINUOUS BONE ARTICULATIONS
Depending on the tissue type, whicharticulates two bones, continuous
articulations are divided into
fibrous, syndesmoses,
cartilaginous, synchondroses,
osseous, synostoses.
6.
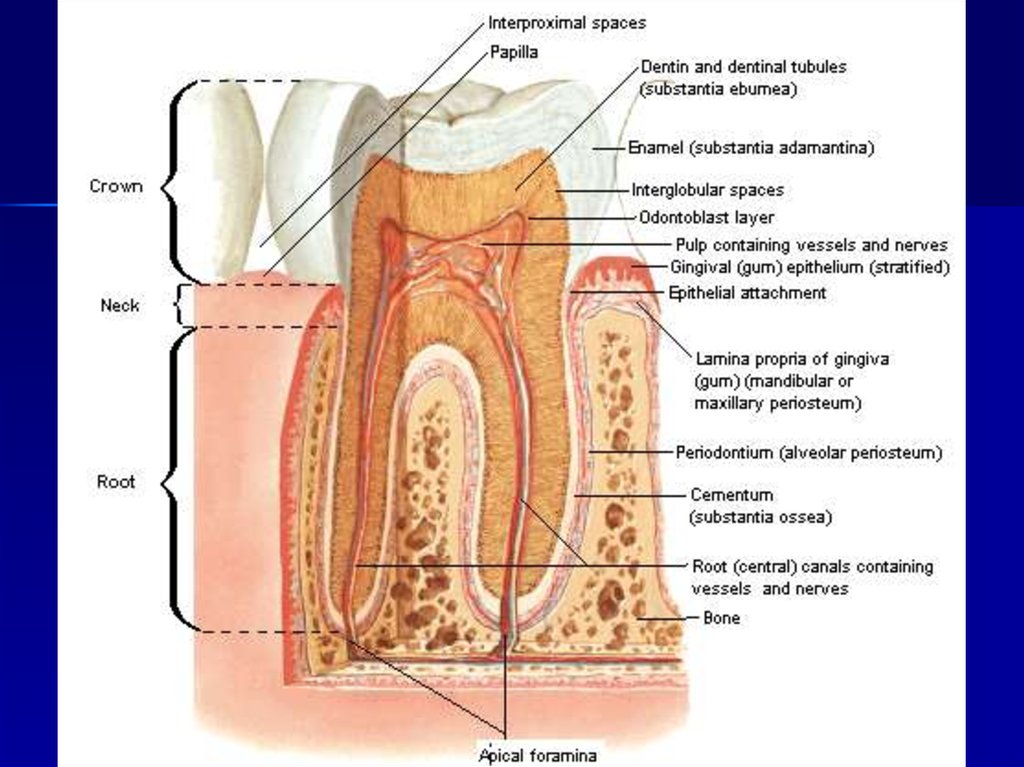
7. Syndesmoses, syndesmosis, (juncturae fibrosae) are formed from the fibrous connective tissue and are divided into the following
groups:gomphosis, gomphosis, dentoalveolar syndesmosis, a fibrous articulation
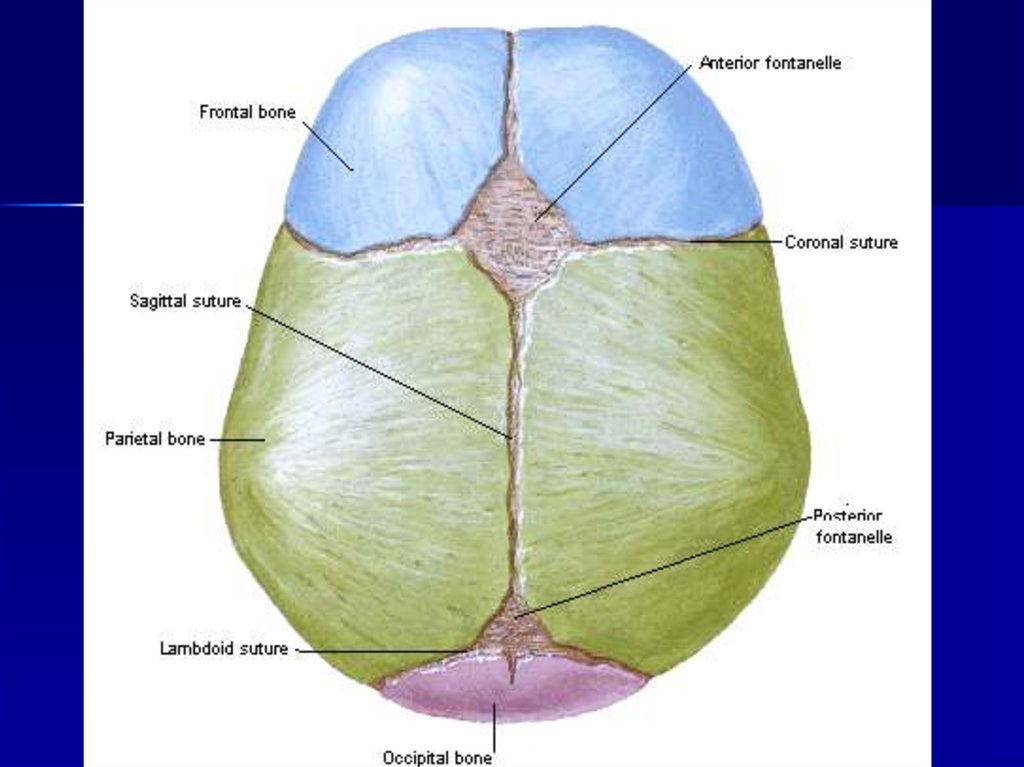
sutures, sutura, fibrous articulations between the bones of the skull, which
fontanelles, fonticuli, between bones of skull of the new-born;
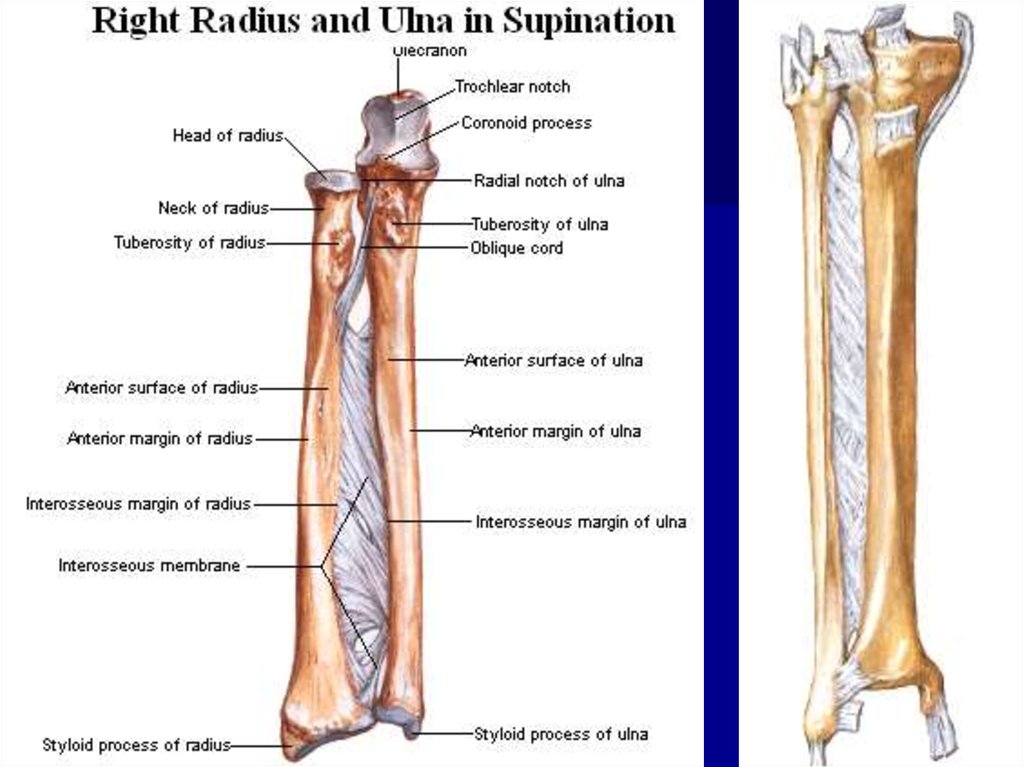
interosseous membranes, membranae interosseae;
ligaments, ligamenta, most of the ligaments consist of a dense regular
between the periodontium of alveolar socket and the root of the tooth;
contain a thin layer of connective tissue;
connective tissue. Fibers in the ligaments run obliquely and cross over like
in the rope. Therefore, ligaments are quite resilient. Collagen fibers of the
ligaments, besides resiliency, provide great elasticity. Some ligaments,
besides collagen fibers, contain a considerable amount of elastic tissue
yellow in color. They are characterized by lower resilience but greater
elasticity. They perform a shock-absorbing function (e.g. yellow ligaments
of the vertebral column). Because of their low resilience, elastic ligaments
are not very common in the body.
8.
9.
10.
11.
12. SYNCHONDROSES:
ACCORDING TOTHE DURATION OF
THE EXISTENCE :
1—TEMPORARY— exist
only to the definite
age.
2—PERMANENT— exist
throughout the life.
ACCORDING TO THE
PROPERTY OF THE
CARTILAGINOUS
TISSUES :
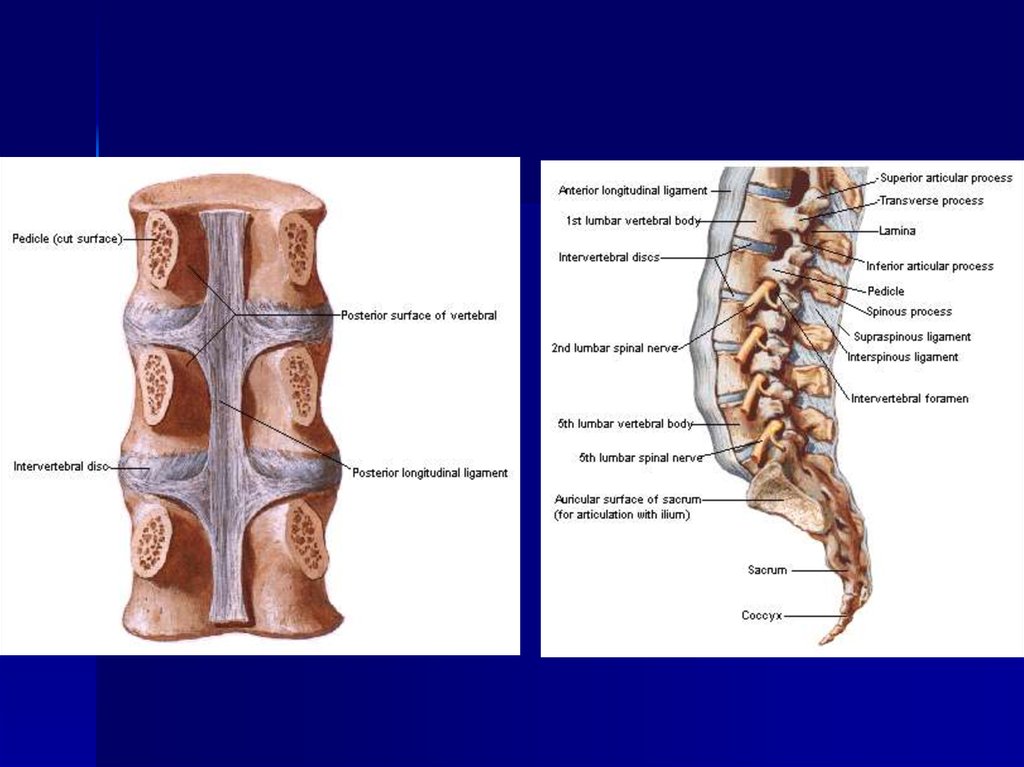
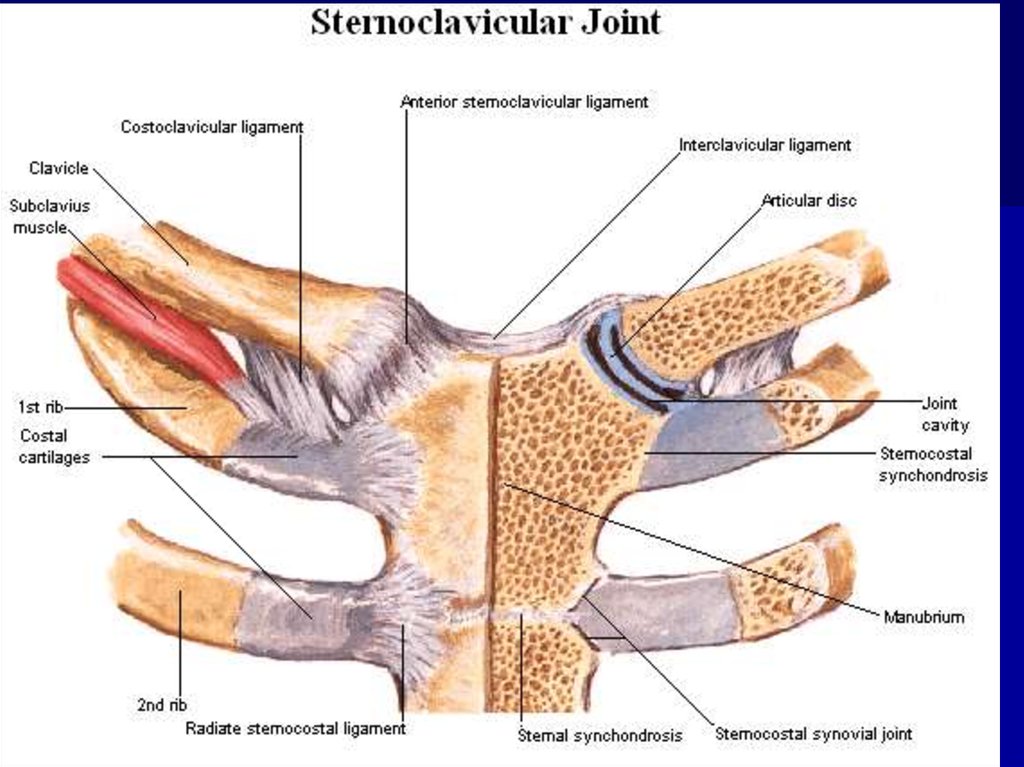
1—HYALINE— between I
rib and sternum.
2—FIBROUS—between
vertebral bodies.
These cartilages have
no vessels and nerves.
13.
14.
15.
When ossified, synchondrosis can betransformed into the osseous articulation
synostosis (synostosis).
Synostoses or bone articulations
(junctura ossea) is contiguous joining of
bones by means of bone tissue, for
instance, synostoses between three bones
of the hip bone in an adult.
16. SYNOVIAL JOINTS
The synovial articulations (juncturaesynoviales, articulatio, diarthrosis) are
discontinuous joints characterized by the
presence of the synovial membrane. They
are also characterized by a variety of
movement amplitudes. Consequently these
joints are most common in higher
vertebrates and humans.
17. THE MOST TYPICAL FEATURES OF THE JOINTS
Each joint possesses four basic elements:articular surfaces, facies articulares;
articular capsule, capsula articularis;
articular cavity, cavitas articularis
hermetically sealed, cleft-like cavity;
between the articulating bones.
synovial fluid
18.
19.
Articular surfaces. The articular surfaces of the bones arecovered with the hyaline cartilage (sometimes fibrous), which is 2.5
mm thick on average. The thickness of the cartilage depends on the
amount of compression experienced by the joint. The surface of the
cartilage is not covered with the perichondrium. The surface is
smooth lubricated with the synovial fluid which reduces friction to
minimum and facilitates the movement.
Articular capsule. The capsule of the joint attaches to the
edges of articular surfaces or somewhat over them. The articular
capsule hermetically seals the articular cavity and consists of two
layers - external fibrous layer, membrana fibrosa, and internal
synovial layer, membrana synovialis.
The fibrous layer of the capsule has a mechanical function. It
consists of bundles of resilient connective tissue fibers, which attach
to the bone penetrating it in the form of Sharpie's fibers.
Synovial membrane. This layer of the articular capsule is a thin
connective tissue membrane, which is lined on the inside with
squamous synovial cells of mesenchymatous origin. Consequently,
the synovial membrane can form folds and protrusions.
20.
Synovial folds and bursae. The synovial membrane is well developedand, in the majority of the joints forms large folds, plicae synoviales,
which contain adipose tissue. They go into the articular cavity, filling its
potential spaces and forming cushions, which absorb shock during motion.
In certain regions, most frequently in the areas of muscular tendons, the
synovial membrane protrudes through the clefts in the fibrous layer and
forms synovial bursae. They serve to reduce friction during tendons'
movement and can be attributed to the accessory muscular apparatus.
Synovial villi. The synovial layer bears numerous, microscopic, synovial
villi, villi synoviales, which significantly increase its surface area, contain
capillary networks, and produce the synovial fluid.
Synovial fluid. In the articular cavity there is a small amount of pale,
thick, synovial fluid. It is produced by the synovial membrane. The synovial
fluid lubricates the articular surfaces and reduces friction between them.
Synovial cavity. Under normal circumstances, the synovial cavity is a thin
cleft, bounded by the synovial membrane and the articular surfaces.
Between the latter, there is a thin layer of synovial fluid, which separates
articulating surfaces. In the pathological processes, the synovial cavity can
accumulate large amounts of inflammatory liquid and greatly increases in
size.
21.
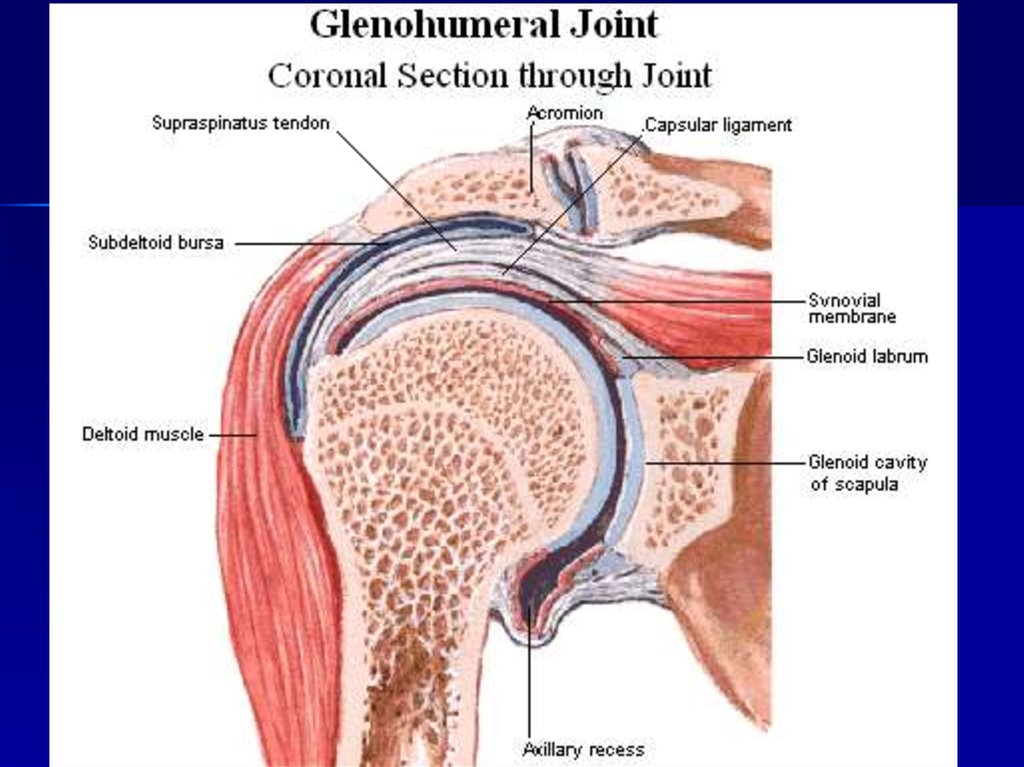
Accessory structures of jointsSynovial joints may possess several accessory elements, which
facilitate movement to a certain extent:
articular disc, discus articularis, a cartilaginous plate, which
completely separates the joint into two regions;
articular meniscus, meniscus articularis, cartilaginous semilunar
plate, which partially separates the synovial cavity;
articular lip, labrum articularis, a cartilaginous rim or lip, which
deepens the articular socket;
intraarticular ligaments, ligg. intraarticularia, connect bones
within the joint; they are covered with the synovial membrane.
Auxiliary strengthening apparatus of joints –
ligaments and tendons of muscles. There are extra-articular and
intra- articular ligaments, covered by synovial membranes.
22. Factors, which aid in the stabilization of articular surfaces:
The fibrous capsule, which is reinforced by theligaments;
Muscles, which surround the joint and actively hold
the bones together due to a constant muscle tone;
Molecular attraction of articular surfaces, lubricated
by the synovial fluid.
23. Congruent and incongruent joints
In those cases, when articulating surfaces entirelycorrespond to each other and appear as imprints of one
another, joints are called congruent (congruo - correspond).
In such joints, articular surfaces are tightly joined together as,
for example, in the hip joint, in which movements are largely
restricted.
Incongruent joints have a greater degree of freedom in
their movements due to the incomplete correspondence of the
articulating surfaces. These joints possess accessory
structures such as disks, menisci, synovial folds, which fill the
irregularities in the articular surfaces and smooth out their
incongruence. The knee joint is an example of the
incongruent joint.
24. Movements in the joints
The frontal axis runs through the joint from right to left.Flexion (flexio) and extension (extensio) of the shoulder occur
around the frontal axis.
The sagittal axis is drawn from front to back. Abduction
(abductio) and adduction (adductio) of the shoulder occur
around this axis.
The vertical axis runs through the joint and through the entire
arm from the top to the bottom. Medial and lateral rotations
(rotatio) of the humerus occur around this axis.
Circumduction (circumductio) takes place when the movement
passes from one axis to another, as when the hand moves in
a circular path. Circular movements are possible in multi-axial
and bi-axial joints.
25. CLASSIFICATION OF JOINTS
Classification of the joints based on thenumber of articulating surfaces:
simple - is composed of only two articulating surfaces;
compound - contains more than two articulating surfaces;
complex joint - if a joint contains articular discs or menisci,
which divide it into two parts;
combined joints - two isolated joints, in which movements
occur simultaneously.
26.
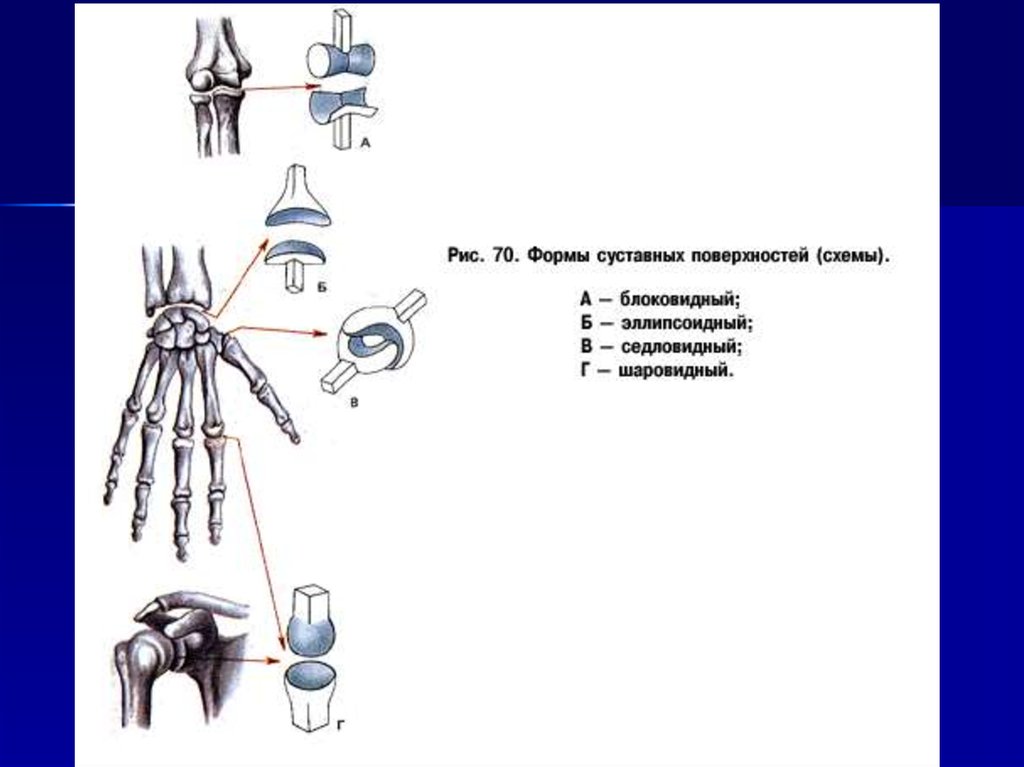
Classification of the joints based on the shape ofarticulating surfaces:
Uni-axial joints
Bi-axial joints
Multi-axial joints
27.
Uni-axial joints. In these joints, movement is restricted toa single axis. There are two types of uni-axial joints:
hinge joint, ginglymus, contains articulating surfaces, which
resemble hinges (for example, interphalangeal joints of the hand
and foot);
pivot joint, art. trochoidea (art. cylindrica), a cylindrical joint,
formed by the convex and concave articulating surfaces cylindrical
in shape (for example, proximal and distal radio-ulnar joints).
28.
Bi-axial joints. These joints permit movements aroundtwo axes, which are perpendicular to each other. The following biaxial joints are distinguished based on their shape:
ellipsoid joint, art. ellipsoidea, contains elliptical (egg-shaped)
articulating surfaces
(for example, radiocarpal joint);
bicondylar joint, art. bicondylaris, consists of a pair of convex,
saddle joint, art. sellaris, contains two articulating surfaces each of
ellipsoid, articulating surfaces, which are rather prominent. Hence,
they are known as condyles (for example, knee joint);
which resembles a saddle
(for example, carpometacarpal joint of the thumb).
29.
Multi-axial joints includejoints and their variations.
spheroidal
Even though, in principle, movements in these joints arc
possible around multiple axes drawn through the joint, rotation
occurs only around three axis:
spheroidal joint (ball-and-socket joint), art. spheroidea, consists of
plane joint, art. plana, contains two flat surfaces, which can be
a globular head and a corresponding concavity. A typical example is
the shoulder joint. Variation of the ball-and-socket joint is the
cotyloid joint. Its head resides in a deep articular socket,
consequently, it is known as the cup-like joint (art. cotylica);
viewed as surfaces of a sphere with a large diameter. Because of
the small size difference of both articulating surfaces, only slight
translations are possible in plane joints (for example, sacroiliac
joint).
30.
31. Clinical applications
Pathological process can develop in the joints,among which infectious arthritis is the most common
(particularly,
rheumatic
or
tuberculous
arthritis).
Inflammations of the synovial membrane — synovitis and
bursitis are also fairly common. Joint deformations,
contraction of the synovial cleft, and restriction of movements
accompanied by pain syndrome can occur as a consequence
of degenerative changes (arthrosis). Traumas can cause
various joint dislocations with stretched and ruptured
ligaments. Physician of different specialties often have to deal
with the diseases of joints.
32.
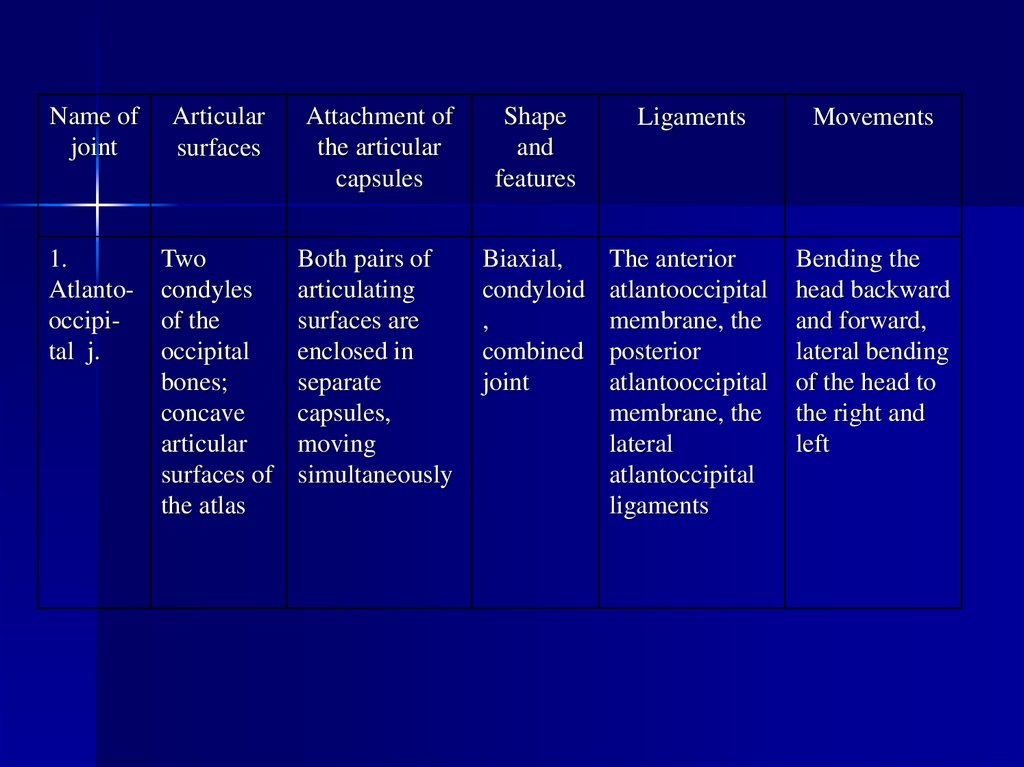
Name ofjoint
Articular
surfaces
Attachment of
the articular
capsules
Shape
and
features
Ligaments
Movements
1.
Atlantooccipital j.
Two
condyles
of the
occipital
bones;
concave
articular
surfaces of
the atlas
Both pairs of
articulating
surfaces are
enclosed in
separate
capsules,
moving
simultaneously
Biaxial,
condyloid
,
combined
joint
The anterior
atlantooccipital
membrane, the
posterior
atlantooccipital
membrane, the
lateral
atlantoccipital
ligaments
Bending the
head backward
and forward,
lateral bending
of the head to
the right and
left
33.
34.
Nameof joint
Articular
surface
Attachment
of the
articular
capsules
Shape
and
features
Ligaments
Movements
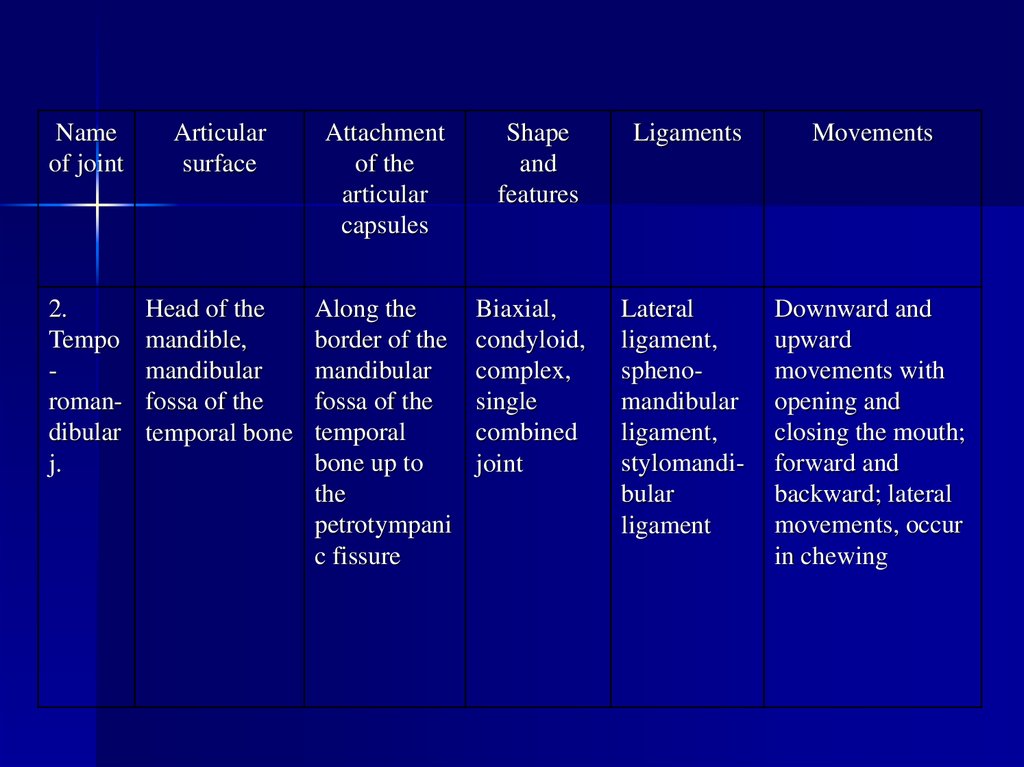
2.
Tempo
romandibular
j.
Head of the
mandible,
mandibular
fossa of the
temporal bone
Along the
border of the
mandibular
fossa of the
temporal
bone up to
the
petrotympani
c fissure
Biaxial,
condyloid,
complex,
single
combined
joint
Lateral
ligament,
sphenomandibular
ligament,
stylomandibular
ligament
Downward and
upward
movements with
opening and
closing the mouth;
forward and
backward; lateral
movements, occur
in chewing
35.
36.
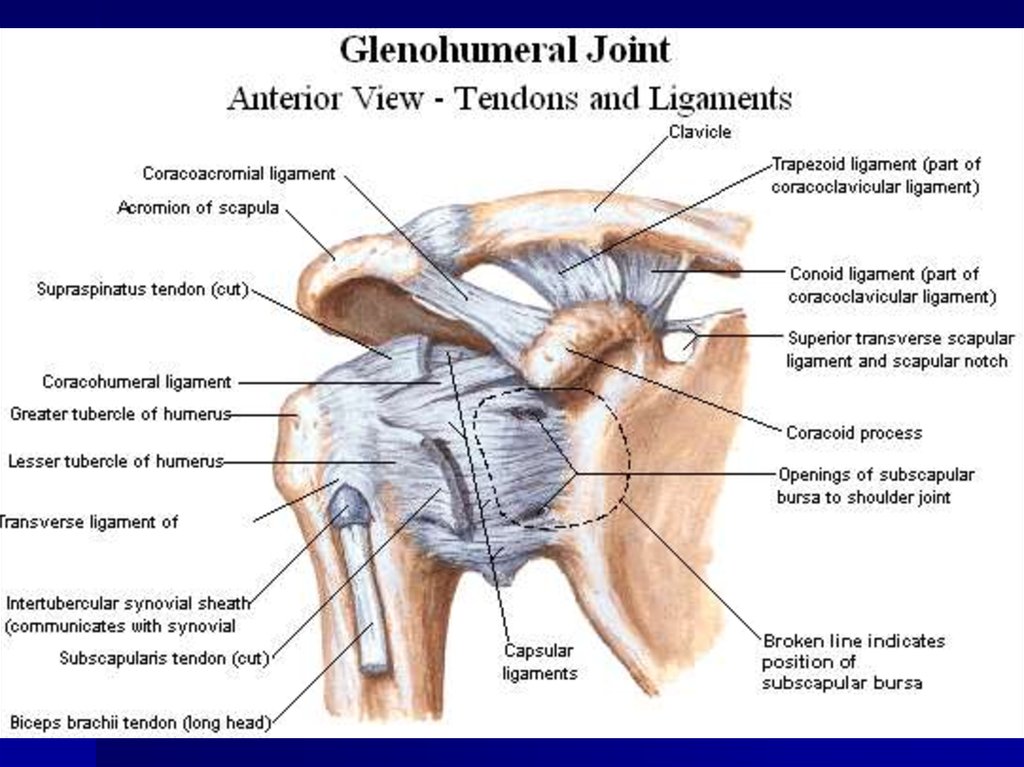
37.
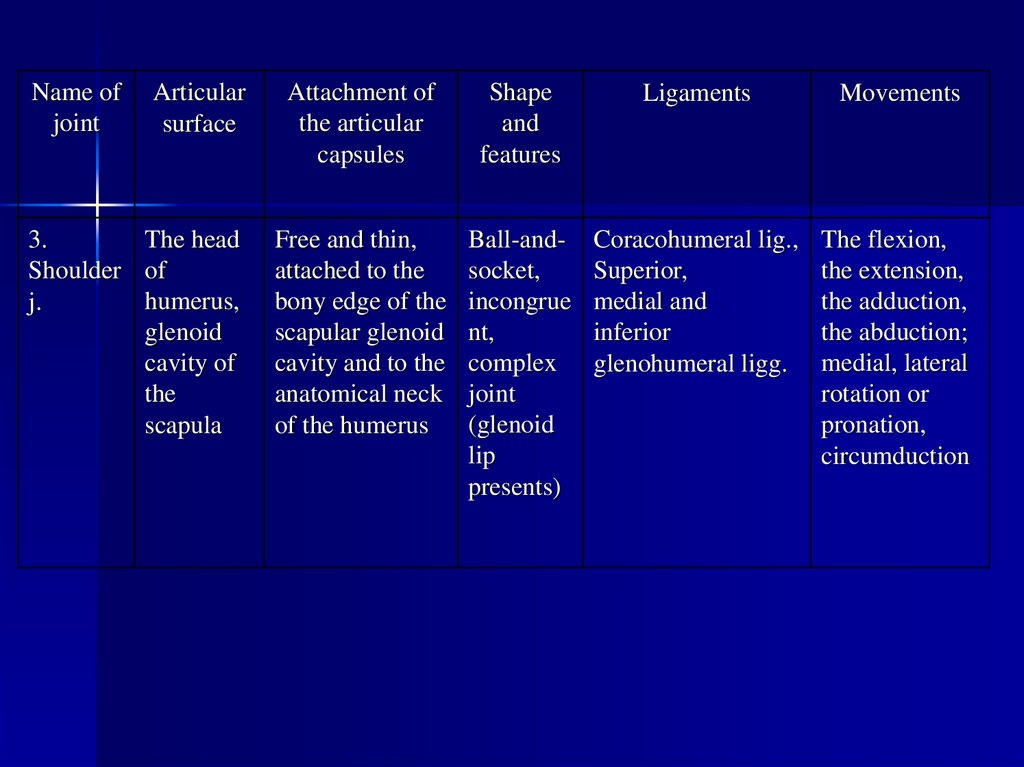
Name ofjoint
Articular
surface
3.
The head
Shoulder of
humerus,
j.
glenoid
cavity of
the
scapula
Attachment of
the articular
capsules
Shape
and
features
Ligaments
Movements
Free and thin,
attached to the
bony edge of the
scapular glenoid
cavity and to the
anatomical neck
of the humerus
Ball-andsocket,
incongrue
nt,
complex
joint
(glenoid
lip
presents)
Coracohumeral lig.,
Superior,
medial and
inferior
glenohumeral ligg.
The flexion,
the extension,
the adduction,
the abduction;
medial, lateral
rotation or
pronation,
circumduction
38.
39.
40.
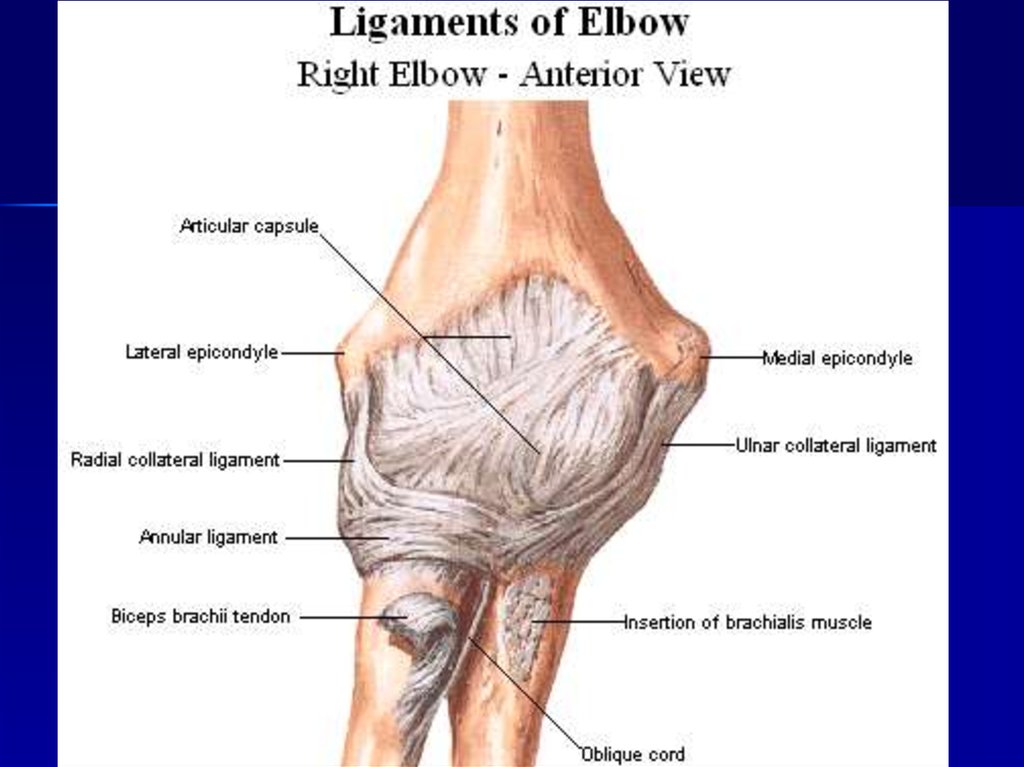
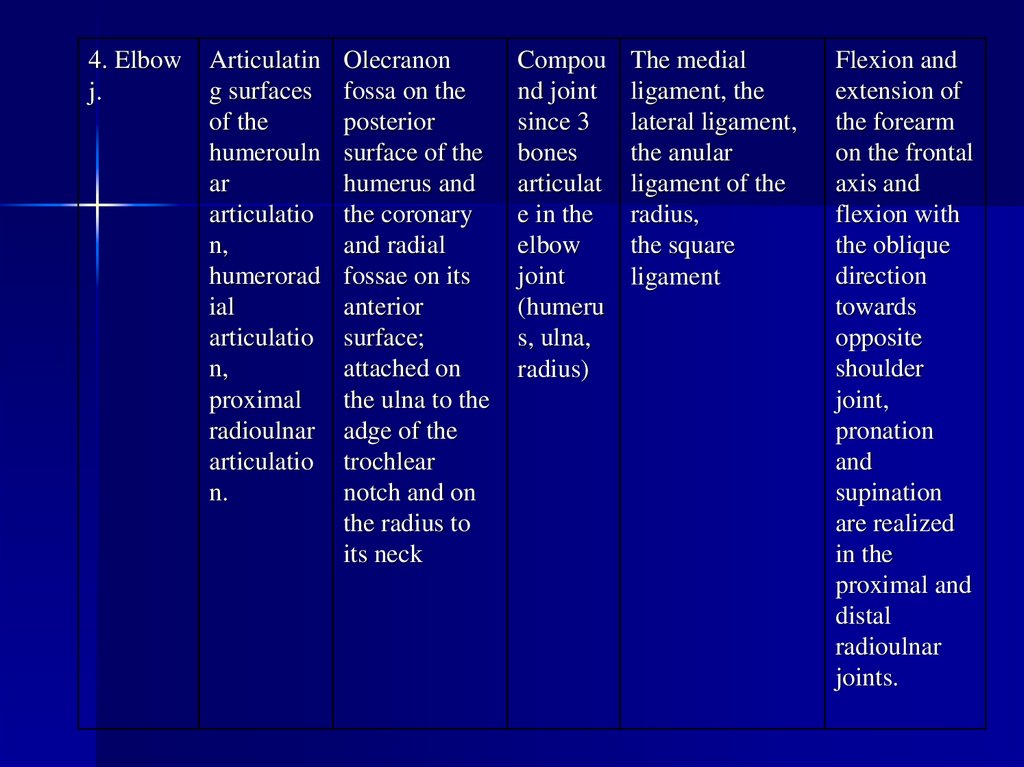
4. Elbowj.
Articulatin
g surfaces
of the
humerouln
ar
articulatio
n,
humerorad
ial
articulatio
n,
proximal
radioulnar
articulatio
n.
Olecranon
fossa on the
posterior
surface of the
humerus and
the coronary
and radial
fossae on its
anterior
surface;
attached on
the ulna to the
adge of the
trochlear
notch and on
the radius to
its neck
Compou
nd joint
since 3
bones
articulat
e in the
elbow
joint
(humeru
s, ulna,
radius)
The medial
ligament, the
lateral ligament,
the anular
ligament of the
radius,
the square
ligament
Flexion and
extension of
the forearm
on the frontal
axis and
flexion with
the oblique
direction
towards
opposite
shoulder
joint,
pronation
and
supination
are realized
in the
proximal and
distal
radioulnar
joints.
41.
42.
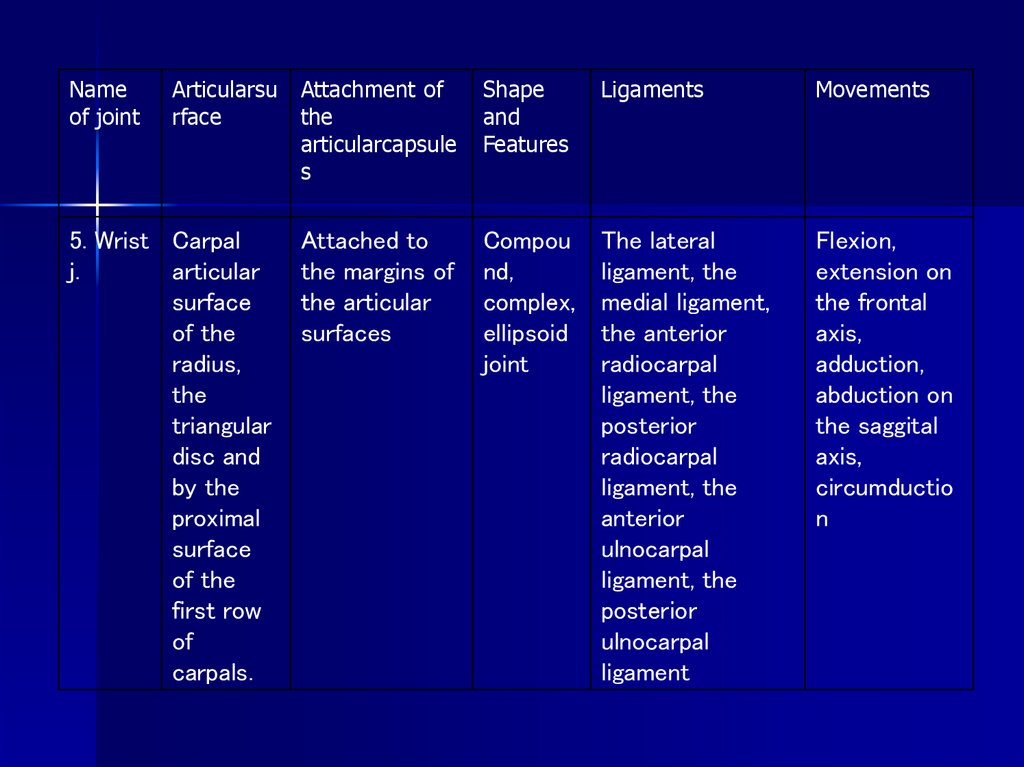
Nameof joint
Articularsu Attachment of
rface
the
articularcapsule
s
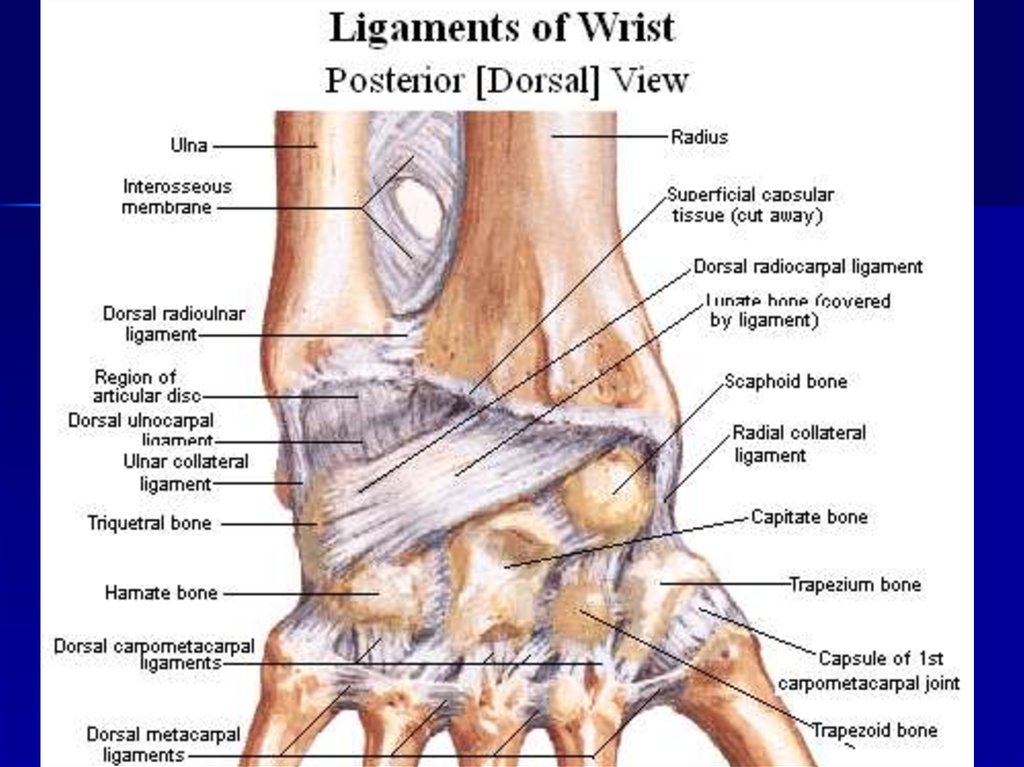
5. Wrist Carpal
j.
articular
surface
of the
radius,
the
triangular
disc and
by the
proximal
surface
of the
first row
of
carpals.
Attached to
the margins of
the articular
surfaces
Shape
and
Features
Ligaments
Movements
Compou
nd,
complex,
ellipsoid
joint
The lateral
ligament, the
medial ligament,
the anterior
radiocarpal
ligament, the
posterior
radiocarpal
ligament, the
anterior
ulnocarpal
ligament, the
posterior
ulnocarpal
ligament
Flexion,
extension on
the frontal
axis,
adduction,
abduction on
the saggital
axis,
circumductio
n
43.
44.
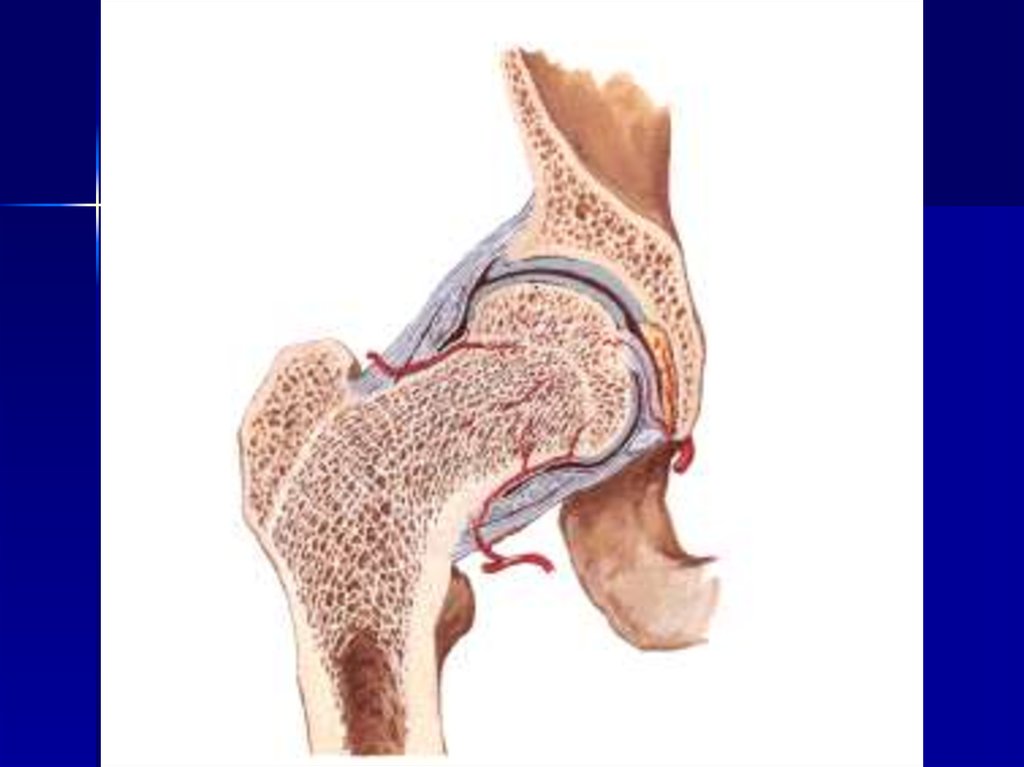
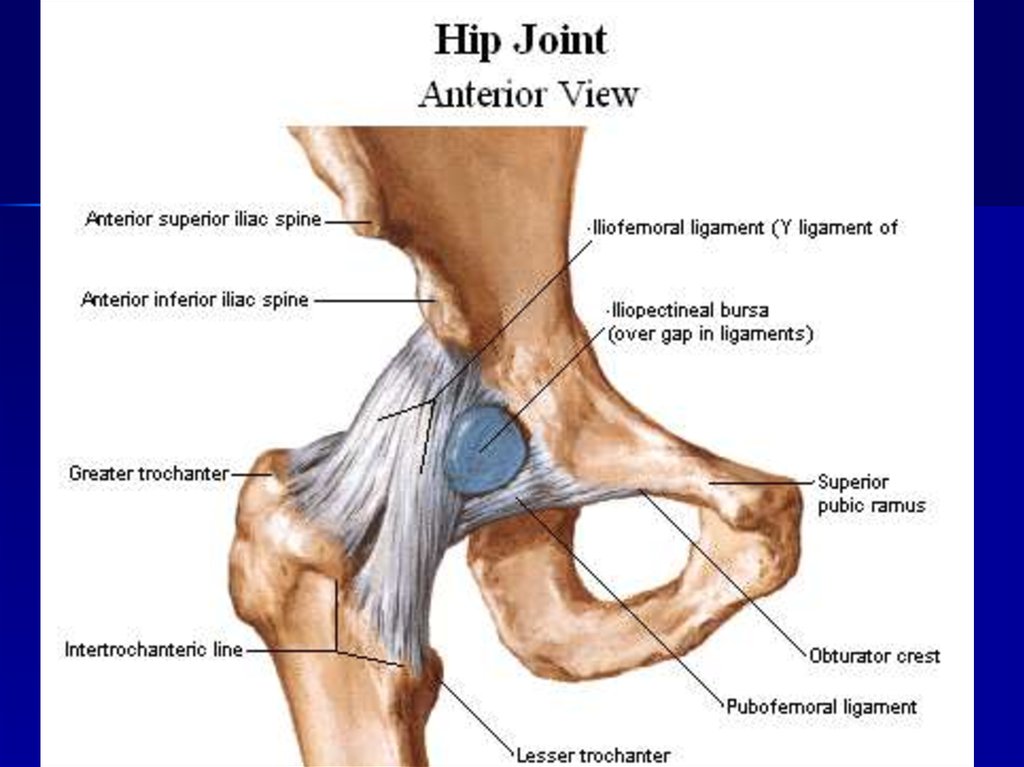
6. Hip j.Cup-like
acetabulu
m of the
hip bone
and the
femoral
head
fitting into
it, a
fibrocartil
aginous
ring
presents.
Attached along
the whole rim
of the
acetabulum
and transverse
ligament of the
acetabulum, to
the femur in
front along the
intertrochanteri
c line and
behind to the
femoral neck
parallel to and
medial of the
intertrochanteri
c crest
Ballandsocket
joint of
the
limited
typecotyloid
joint,
complex
joint.
Extraarticular
ligaments:
the iliofemoral lig.,
the pubofemoral
lig.,
the ischiofemoral
lig.,
the orbicular zone.
Intraarticular
ligaments:
the transversum
acetabular lig.,
the lig. of the
femur`s head.
Flexion (to
the front),
extension (to
the back);
abduction,
adduction;
limited
circumduction
45.
46.
47.
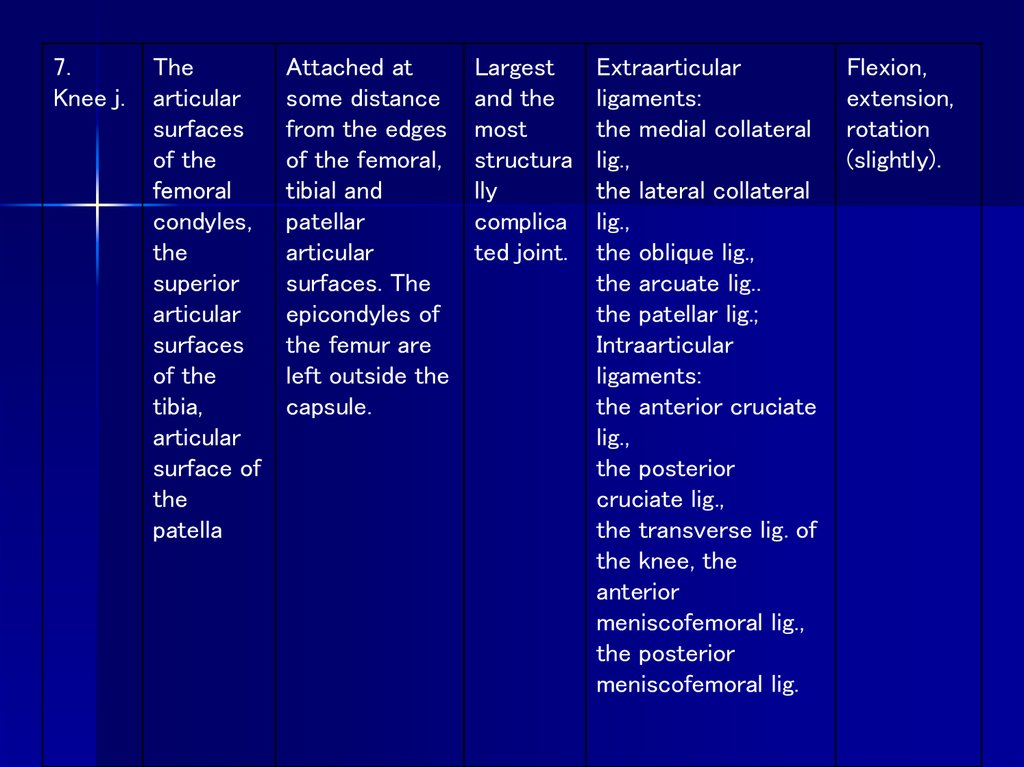
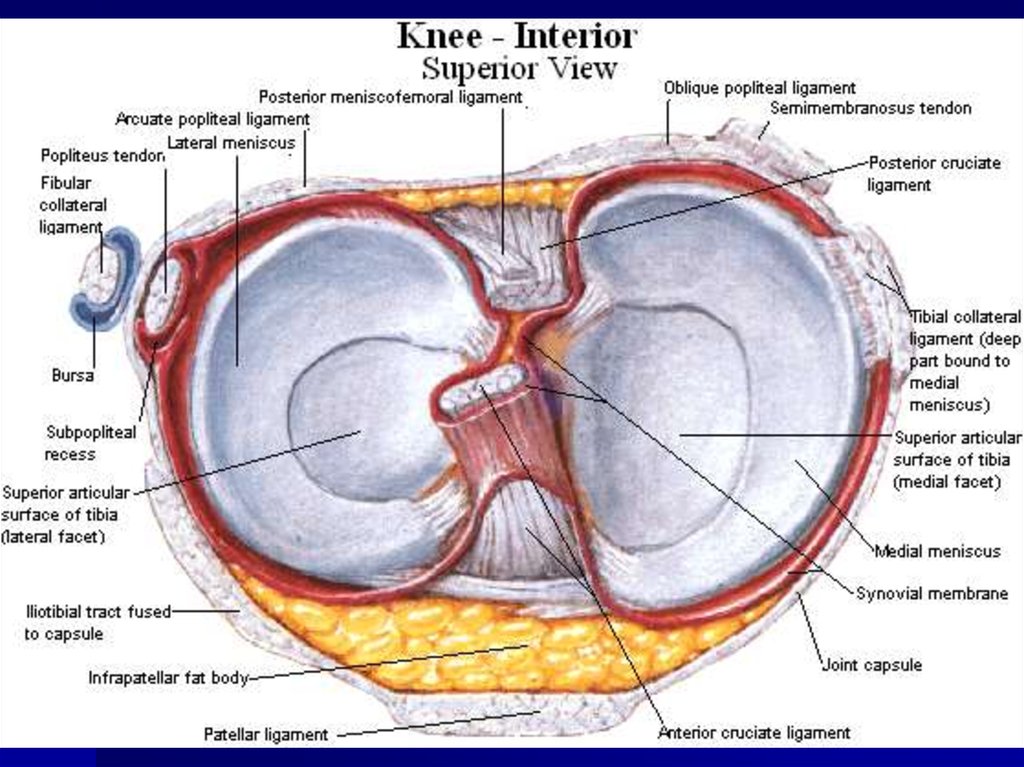
7.Knee j.
The
articular
surfaces
of the
femoral
condyles,
the
superior
articular
surfaces
of the
tibia,
articular
surface of
the
patella
Attached at
some distance
from the edges
of the femoral,
tibial and
patellar
articular
surfaces. The
epicondyles of
the femur are
left outside the
capsule.
Largest
and the
most
structura
lly
complica
ted joint.
Extraarticular
ligaments:
the medial collateral
lig.,
the lateral collateral
lig.,
the oblique lig.,
the arcuate lig..
the patellar lig.;
Intraarticular
ligaments:
the anterior cruciate
lig.,
the posterior
cruciate lig.,
the transverse lig. of
the knee, the
anterior
meniscofemoral lig.,
the posterior
meniscofemoral lig.
Flexion,
extension,
rotation
(slightly).
48.
49.
50.
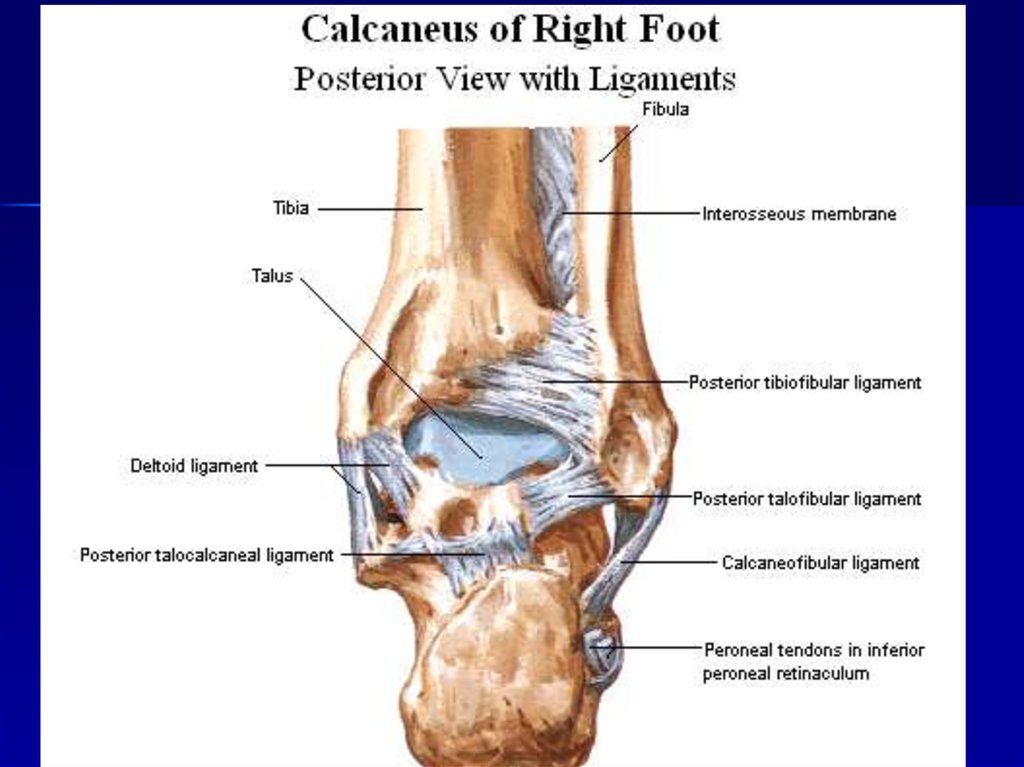
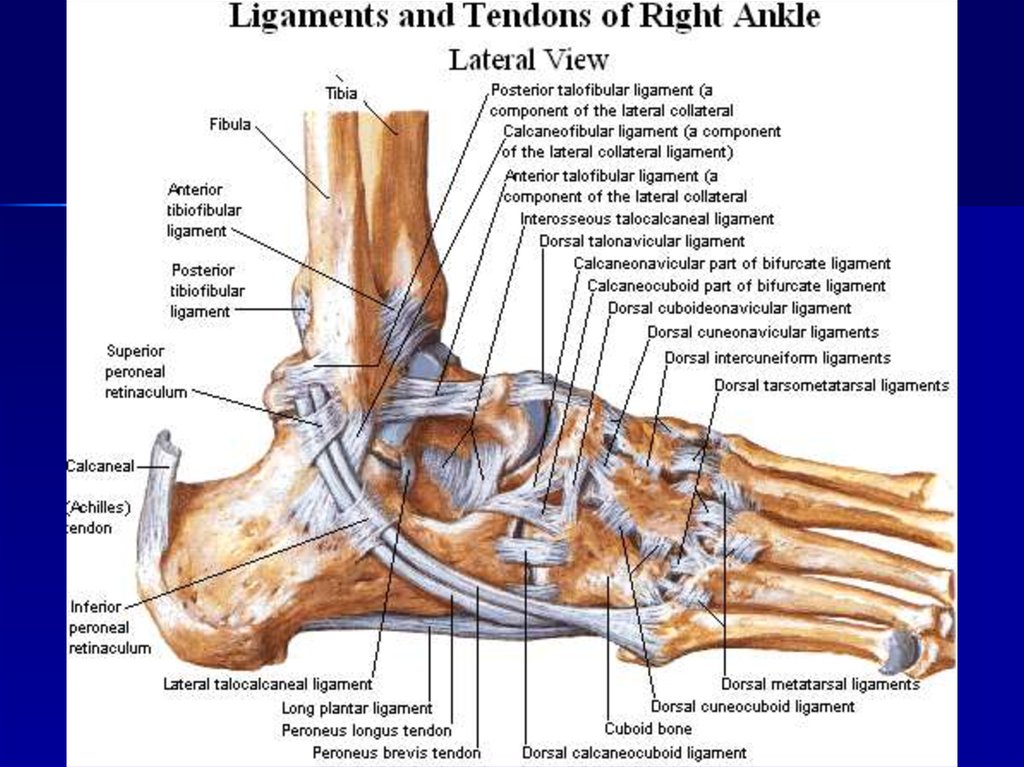
8. Ancle Lowerj.
articular
surfaces
of the
tibia and
its
malleolus,
the
articular
surfaces
of the
malleolus
of the
fibula, the
articular
surfaces
of the
trochlea
of the
talus
Attached to the
cartilaginous
margins of the
articular
surfaces,
covers part of
the talus neck
in front.
Compoun
d joint,
the
shape is
hinge
The lateral
ligament consists
of: the anterior
talofibular lig.,
the posterior
talofibular lig., the
calcaneofibular lig.;
The medial
(deltoid) ligament
consists of: the
anterior and
posterior
tibiotalar lig.,
tibiocalcaneus lig.,
tibionavicular lig.
The foot
raises with
toes upwards
(dorsiflexion
or extension)
or lowers
(plantar
flexion), slight
side
movements
(on plantar
flexion).
51.
52.
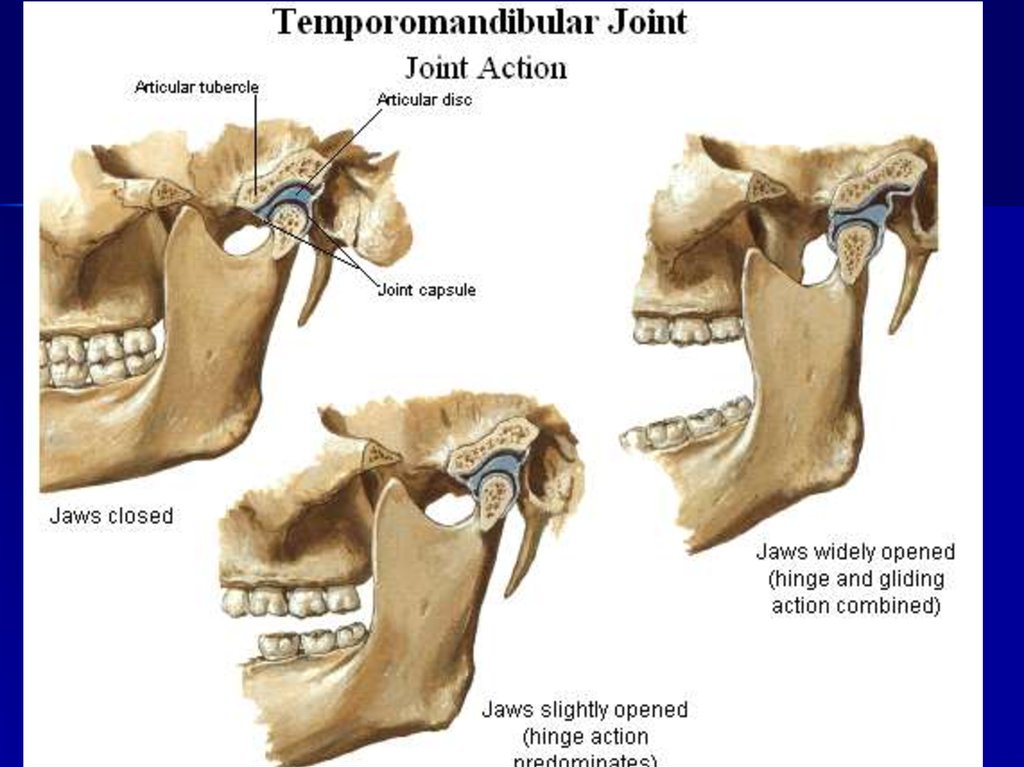
53. THE TEMPOROMANDIBULAR JOINT
The temporomandibular joint, articulatio temporomandibularis, ispaired and formed by the articulation of the head of the mandible
(ellipsoid in shape) with the mandibular fossa of the temporal bone.
It belongs to the group of the bicondylar, combined joints.
The articular surfaces are incongruent. Therefore, inside the joint
there is the articular disk, discus articularis, which fuses with the
fibrous capsule and divides the articular cavity of the joint into two
isolated levels - the upper and the lower (complex joint).
Fibrous capsule. In the region of the temporal bone, the capsule
is attached to the margins of the mandibular fossa, fossa
mandibularis, covers in the front the articular tubercle,
tuberculum articulare, and in the back reaches the
petrotympanic fissure. On the mandible, the capsule attaches to the
edge of the articular surface of the head in the front (above the
pterygoid fossa), while in the back it inserts into the neck of the
mandible.
54.
Ligaments.The capsule is reinforced by the lateral ligament, lig. laterale, whose fibers
run obliquely from the zygomatic process of the temporal bono to the neck
of the mandible. Importantly, (ho following fasciae (ligaments) thicken in
order to stabilize the mandible:
1) lig. stylomandibular, which runs from the styloid process of the temporal
bone to the posterior angle of the mandible;
2) lig. sphenomandibulare, which extends from the spine of the sphenoid
towards the lingula of the mandible.
Movements. The temporomandibular joint permits the following
movements:
1) elevation and depression of themandible occurs around the frontal axis
in the lower level of the joint. When the mandible is exceedingly depressed,
the articular disk with the head of the mandible may be displaced onto the
articular tubercle;
2) protrusion of the mandible occurs in the upper level of the joint in such a
way that the head together with the articular disk are drawn onto the
articular tubercle;
3) lateral movements of the mandible occur such that on one side the head
remains in the fossa, whereas on the opposite side it: is drawn onto the
articular tubercle together with the articular disc.
55.
MASTICATORY MUSCLESThe masticatory muscles are derived from the common mesenchymatous primordium of the
first visceral (mandibular) arch, which is associated with the third branch of the trigeminal
nerve. All of the masticatory muscles (four) act on the temporomandibular joint and move the
mandible. They can be divided into the superficial and deep muscles .
THE SUPERFICIAL MASTICATORY MUSCLES
Masseter, m. masseter.
Origin: zygomatic arch.
Insertion: masseteric tuberosity and angle of the mandible. It consists of two parts —
superficial (pars superficialis) and deep (pars profunda).
Action. Elevates the mandible; the superficial part protracts the mandible.
Temporalis, m. temporalis.
Origin: temporal and parietal bones, temporal fascia.
Insertion: coronoid process of the mandible. The muscle fills the temporal fossa. It is flat and
fan-shaped. The anterior fibers of the temporalis are directed vertically, middle fibers —
obliquely, and posterior fibers — almost horizontally. The fibers of the muscle converge below
forming a thick tendon, which runs underneath the zygomatic arch and inserts into the
coronoid process.
Action. Elevates and retracts the mandible.
56.
THE DEEP MASTICATORY MUSCLESMedial pterygoid, m. pterygoideus medialis.
Origin: pterygoid fossa of the pterygoid process.
Insertion: pterygoid tuberosity of the mandible.
Action. Elevates and pulls the mandible to the side. When the muscle contracts on both
sides, it protracts the mandible.
Lateral pterygoid, m. pterygoideus lateralis.
Origin: arises by two heads: from the infratemporal crest of the sphenoid bone (upper
head) and lateral plate of the pterygoid process (lower head).
Insertion: pterygoid fossa of the neck of the mandible and capsule of the
temporomandibular joint.
The muscle is triangular in shape. Its fibers are directed backward and laterally. It lies
deep in the infratemporal fossa covered by the zygomatic arch and the ramus of the
mandible as well as by the temporal muscle.
Action. In unilateral contraction, the muscle moves the mandible to the opposite side;
when the lateral pterygoid muscles of the two sides act together they protrude the
mandible.
Nerve supply of the masticatory muscles. All masticatory muscles arc supplied by the
third branch of the trigeminal nerve.
57.
Muscles of the neckIs divided into three groups: - Superficial
- medial or muscles of the hyoid bone
- deep
Superficial Muscles of the neck
1. The platysma is subcutaneous muscle, which attached from the 2 rib to
the mandible.
Action: - pulling the skin of the neck;
- depress the angle of the mouth.
2. The sternocleidomastoid muscle lies under the platysma.
Attached: - the hilt of sternum
- the sternal and of the clavicle
- the mastoid process
- the superior nuchae line.
Action: - hold the head in a vertical position
58.
Middle muscles of the neckIs divided into 2 groups: - above the hyoid bone and below.
Muscles located above the hyoid bone
1.The mylohyoid muscle is flat, connected to the mylohyoid muscle.
2. The digastric muscle consists of two bellies. Anterior arises from the
digastrics fossa, posterior – the mastoid process.
3. The stylohyoid muscle – the styloid process of temporal bone.
4. The geniohyoid muscle – lies above the mylohoid muscle on the mental spine
of mandible.
59.
Muscles located below the hyoid bone1. The sternohyoid muscle attached the hilt of the sternum, sterna and of the
clavicle.
Action: - pulls the hyoid bone downwards.
2. The sternothyroid muscle: - lies under the sternohyoid muscle, lowers the
larynx.
3. The thyrohyoid muscle is continuated of the sternothyroid muscle, pulls the
larynx upwards.
4. The omohyoid muscle – consists of two bellies, inferior and superior. Inferior
arises of the subscapular notch and connected with superior belly.
Action: pulls the hyoid bone downwards.
60.
The Deep muscles of the neckIs divided into three groups: - lateral, attached to the ribs
- prevertebral
- suboccipital
The Deep lateral muscles of the neck
1. The anterior scalene muscle
2. The medius scalene muscle
3. The posterior scalene muscle
They attached the transverse processes of the cervical vertebrae.
Action: raises the upper ribs, inspiration muscles.
The Deep prevertebral muscles of the neck
1. The long muscle of the neck
2. The long muscle of the head
Action: flex the head forward and laterally
The Deep suboccipital muscles of the neck
1, 2. The anterior and lateral straight muscles of the head – flex the head
forward, spine – laterally.
3, 4. The obliquus capitis superior and inferior muscles
5, 6. The greater and lesser straight muscles
Action: rotate the head and pull it backwards.