















Похожие презентации:





")




Breech presentation
1.
Breech presentationPATELIYA BHARGAV
GROUP NO. 163 B
2.
• The definition of breechpresentation is when the
buttocks, foot or feet are
presenting instead of the head
3. classifications
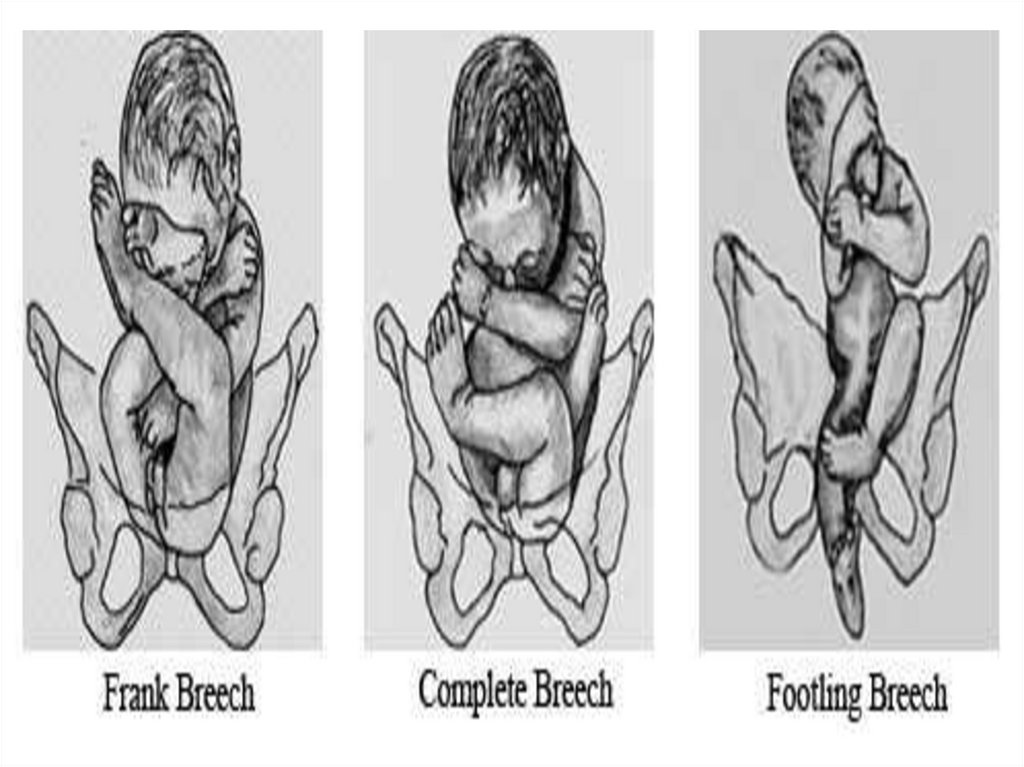
• Frank breech where the hips are flexed andlegs extended
• Complete breech where the hips and knees
are flexed and the feet are not below the level
of the fetal buttocks
• Footling breech where one or both feet are
presenting as the lowest part of the fetus
4.
5.
Associations andCauses
6. Maternal factors
Polyhydraminos
Uterine anomalies (bicornuate, septate)
Space occupying lesions (e.g fibroids)
Placental abnormalities (praevia, cornual)
Multiparity (in particular grand multips)
7. Fetal factors
• Prematurity• Fetal anomalies (e.g neurological,
hydrocephalus, anenecephaly)
• Multiple pregnancy
• Fetal death
• Short umbilical cord
8.
• The incidence of breech presentationdecreases from about 20% at 28 weeks of
gestation to 3–4% at term, as most babies
turn spontaneously to the cephalic
presentation
9.
What information should be givento women with breech
presentation regarding mode of
delivery?
10. Term Breech Trial 2000
• trials with 2396 participant• Caesarean delivery 1060/1169 (91%) of those
women allocated to planned caesarean
section
• 550/1227 (45%) of allocated to a vaginal
delivery protocol
11.
• Perinatal or neonatal death(excluding fatalanomalies) or short-term neonatal morbidity
was reduced with a policy of planned
CS(RR 0.33, 95% CI 0.19–0.56) and perinatal or
neonatal death alone (excluding fatal
anomalies) was reduced with a policy of
planned caesarean section (RR 0.29, 95% CI
0.10–0.86)
12.
• After excluding ,perinatal mortality, neonatalmortality or serious neonatal morbidity with
planned caesarean section compared with
planned vaginal birth was 16/1006 (1.6%)
compared with 23/704 (3.3%) (RR 0.49; CI
0.26–0.91); P = 0.02).
13.
adverse perinatal outcome was lowest withprelabour caesarean section and increased
with caesarean section in labour
14.
• In the latter study, of the 2526 women withplanned vaginal deliveries, 1796 delivered
vaginally (71%)
• The rate of neonatal morbidity or death was
considerably lower than the 5% in the Term
Breech Trial (1.60%; 95% CI 1.14–2.17), and
not significantly different from the planned
caesarean section group
15.
• death or neurodevelopmental delayat age 2years, was similar between the two groups.
16. Summary of TBT
• lower rates of perinatal and neonatal death• lower rates of short term neonatal morbidity
or perinatal death
• fewer 5 minutes Apgar scores <7
• lower risk of adverse perinatal outcomes
• small increase in the short term maternal
morbidity
17. What factors affect the safety of vaginal breech delivery
should be assessedcarefully before
selection for vaginal
breech birth
18. unfavourable for vaginal breech birth
• ● other contraindications to vaginal birth (e.g. placenta praevia,compromised fetal condition)
• ● clinically inadequate pelvis
• ● footling or kneeling breech presentation
• ● large baby (usually defined as larger than 3800 g)
• ● growth-restricted baby (usually defined as smaller than 2000 g)
• ● Hyperextended fetal neck in labour (diagnosed with ultrasound or X-ray
where ultrasound is not available)
• ● lack of presence of a clinician trained in vaginal breech delivery
• ● previous caesarean section.
19. Intrapartum management
• should take place in a hospital with facilitiesfor emergency caesarean section
• Labour induction for breech presentation may
be considered if individual circumstances are
favourable
• Labour augmentation is not recommended
20.
• Epidural analgesia should not be routinelyadvised; women should have a choice of
analgesia during breech labour and birth.
21.
• Continous electronic fetal heart ratemonitoring should be offered to women with
a breech presentation in labour.
• Fetal blood sampling from the buttocks during
labour is not advised.
22.
• Caesarean section should be considered ifthere is delay in the descent of the breech at
any stage in the second stage of labour.
• Episiotomy should be performed when
indicated to facilitate delivery.
23.
• Three types of vaginal breech deliveriesSpontaneous breech delivery
Assisted breech delivery
Total breech extraction
24. Total breech extraction
• only with 2nd nonvextex twin delivery
• procedure in which the
infant's feet are grasped
by the operator and the
fetus is extracted from
the uterine cavity
through the vagina.
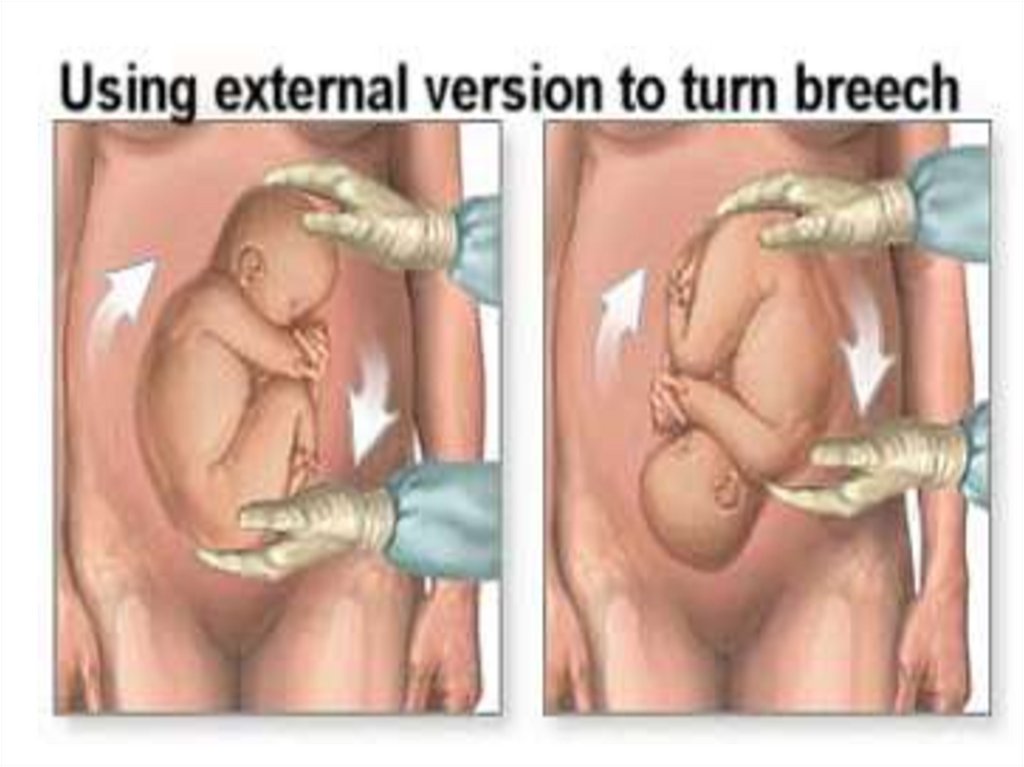
25. ECV
• External cephalic version (ECV) is thetransabdominal manual rotation of the fetus into
a cephalic presentation.
• after ECV successful rate 35-86%
• breech presentation at term, after ECV 1 - 1.5%
• indications for urgent caesarean after ECV 1 - 3%
• The risk of intrauterine death of foetus after ECV
is about 0.0001%
26.
27. contraindication to ECV
preterm
Multiple pregnancy
significant third trimester bleeding
IUGR,
oligohydramnion
PROM
PIH
nonreassuring foetal monitoring patterns
all contraindications to vaginal birth are
concerned to execute ECV
28. Risk of ECV
umbilical cord entanglement
abruptio placenta
premature rupture of the membranes (PROM)
severe maternal discomfort
29.
THANKYOU