")























 Биология
БиологияПохожие презентации:



")
")

")
")

")
Immunophysiology of obesity
1. Immunophysiology of OBESITY (тучность, ожирение)
2.
3.
4.
5.
6.
7.
8.
9.
Adipose tissue depots occur throughout the body. Studies suggest that visceral adipose tissueaccumulation is a major risk factor for cardiometabolic disease, whereas subcutaneous fat seems
to be neutral or protective. Other adipose tissue depots of note include the epicardium, the
perivascular space, and bone marrow, but the functional significance of these tissues is largely
unknown. Brown adipose tissue occurs in the supraclavicular and paraspinal regions. In
contrast to white adipose tissue, brown adipose tissue is metabolically active, and it functions to
utilize fuel to produce heat. In addition, ectopic lipid can accumulate in tissues, such as liver, in
metabolically dysfunctional organisms.
10.
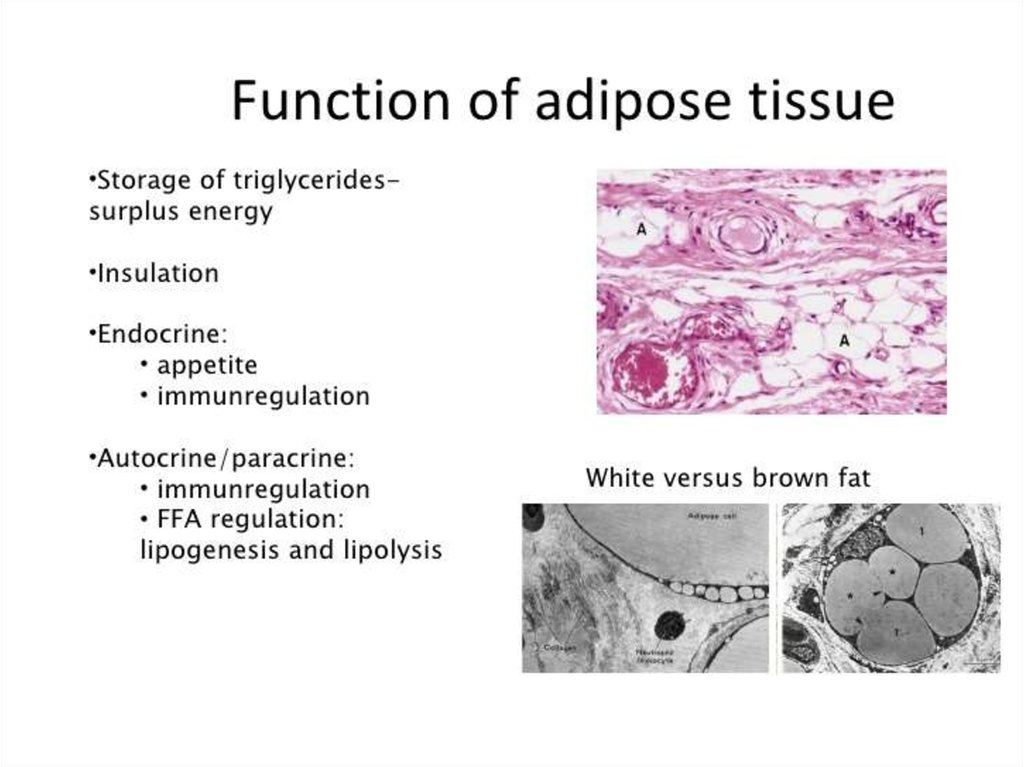
Adipose tissue constitutes an extremely active endocrine organ with a network ofsignaling pathways enabling the organism to adapt to a wide range of different metabolic
challenges, such as starvation (голод), stress, infection, and short periods of gross energy excess.
The functional pleiotropism of adipose tissue relies on its ability to synthesize and release a
huge variety of hormones, cytokines, complement and growth factors, extracellular matrix
proteins, and vasoactive factors, collectively termed adipokines. Obesity is associated with
adipose tissue dysfunction leading to the onset of several pathologies including type 2 diabetes,
dyslipidemia, nonalcoholic fatty liver, or hypertension, among others.
The mechanisms underlying the development of obesity and its associated
comorbidities include the hypertrophy and/or hyperplasia of adipocytes, adipose tissue
inflammation, impaired extracellular matrix remodeling, and fibrosis together with an altered
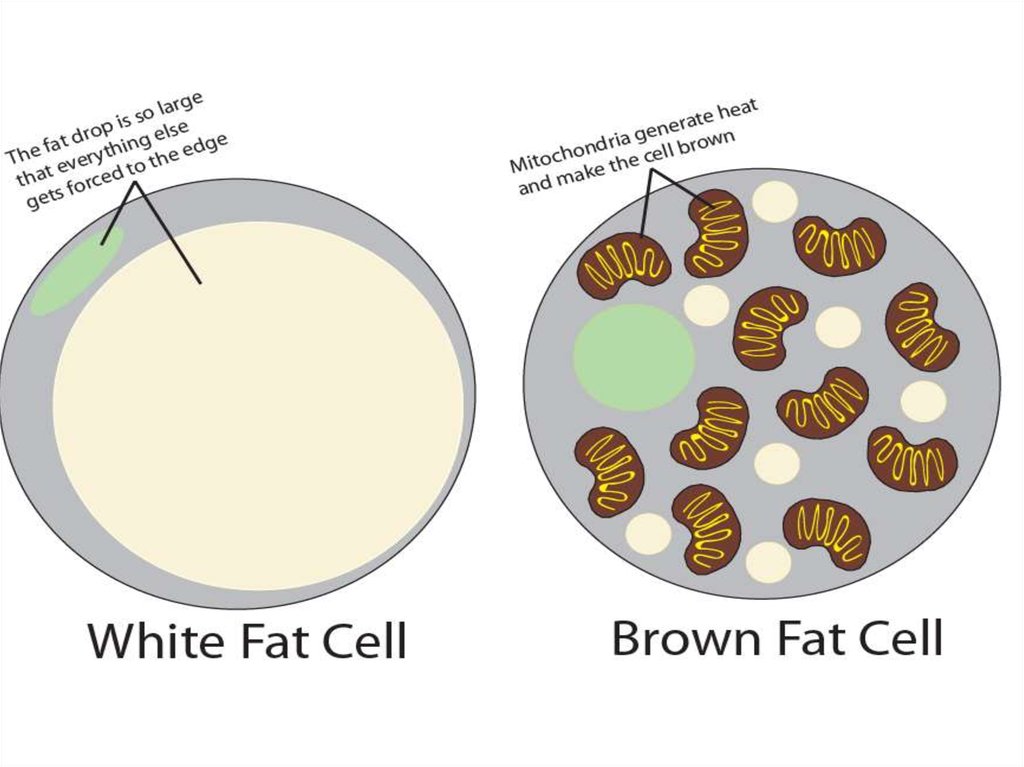
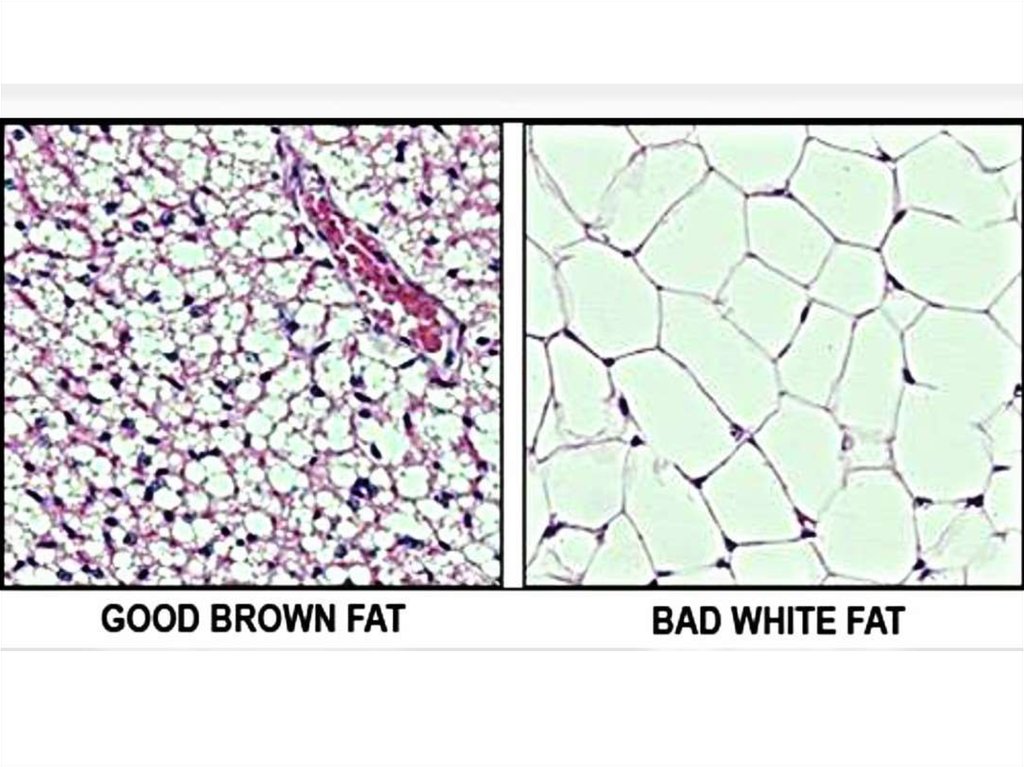
secretion of adipokines. Recently, the potential role of brown and beige adipose tissue in the
protection against obesity has been also recognized. In contrast to white adipocytes, which
store energy in the form of fat, brown and beige fat cells display energy-dissipating capacity
through the promotion of triacylglycerol clearance, glucose disposal, and generation of heat
for thermogenesis. Identification of the morphological and molecular changes in white, beige,
and brown adipose tissue during weight gain is of utmost relevance for the identification of
pharmacological targets for the treatment of obesity and its associated metabolic diseases.
11.
Proteins secreted by the adipocyte. The list of proteins and factors secreted by the adipocyte isgrowing rapidly. Several of these proteins/factors act as endocrine hormones, for example, leptin,
IL-6, whereas others act locally, for example, TNF-a and the growth factors. The endocrine
proteins/factors are proposed to influence distant tissues such as the liver, skeletal muscle or brain
to modulate insulin action, that is, the 'endocrine hypothesis'. Paracrine/autocrine factors may
also modulate insulin action if they promote or inhibit adipocyte proliferation and/or
differentiation.
12.
WAT: white adipose tissue, SAA3: serum amyloid A3, FLS: fibroblast-like synoviocytes, AC:articular chondrocytes, PMN: neutrophils, MMP: metalloprotease, COX-2: cyclooxygenase 2,
ROS: reactive oxygen species, iNOS: inducible nitric oxide synthase, CC-CK: CC-chemokines,
TG2: transglutaminase 2, and TERA: transitional endoplasmic reticulum ATPase.
13.
14.
Recent evidence has also pointed to the heterogeneity of adipose tissue macrophages,that is, M1 or classically activated (pro-inflammatory) macrophages and M2 or
alternatively activated (anti-inflammatory) macrophages. Under lean condition,
adipocytes secrete factors that promote M2 activation of macrophages, such as
interleukin-4 (IL) and interleukin-13 (IL-13). M2 macrophages secrete anti-inflammatory
mediators. On the other hand, adipocytes secrete pro-inflammatory FFAs, chemokines,
and cytokines under obese condition. Activated M1 macrophages produce large
amounts of pro-inflammatory cytokines, thereby accelerating inflammatory responses in
adipose tissue through paracrine interaction between adipocytes and macrophages.
15.
Whereas macrophages in lean mice and humans make up around 5% of the cells inadipose tissue, during obesity they constitute up to 50% of all adipose tissue cells.
16.
17.
18.
Role of the immune system in lean versus obese adipose tissue.In lean adipose tissue, T-helper type 2 (TH2) cells produce anti-inflammatory cytokines such as
interleukin (IL)-4, 10, and 13 which promote alternatively activated M2 macrophage polarization.
M2 polarization is also induced by regulatory T cells (Tregs) and eosinophils via IL-4. M2
macrophages secrete other anti-inflammatory signals such as IL-10 which maintain insulin
sensitivity within lean adipose tissue. Conversely, TH1 type cytokines such as interferon (IFN)γ stimulate M1 macrophage polarization in obese adipose tissue. Other immune cells are also
increased in obese adipose tissue which contribute to insulin resistance including mast cells,
B cells, and immunoglobulins (Igs). CD8(+) T cells promote Adipose tissue macrophages
(ATM) accumulation and proinflammatory gene expression and are also increased as well.
Contrary to the lean state, in which ATMs are distributed throughout the adipose tissue exposing
limited inflammatory properties, ATMs in obese adipose tissue are located around dead
adipocytes and form so-called crown-like structures (CLSs) while displaying profound
proinflammatory features. Macrophage presence in CLSs within obese adipose tissue has been
directly linked with insulin resistance.
M1 macrophages are proinflammatory, secreting cytokines such as TNF-α and IL-1β.
Macrophages are bone-marrow-derived myeloid cells hence both M1 and M2 macrophages
express the myeloid cell surface markers F4/80 and CD11b. However, only the M1 population
expresses the marker CD11c.
19.
20.
• Macrophages play a significant role in regulating adipose tissue functioning duringhealth and disease
• In addition to conventional functions such as clearing cellular debris and participating in
tissue immune surveillance, lipid buffering is an important function of ATMs
• Obesity-induced inflammation, characterised by an elevated number of
proinflammatory macrophages in adipose tissue, has been suggested to contribute to
systemic insulin resistance
• Their origin, as well as a combination of peripheral changes and adipose tissue-derived
stressors, probably contribute to ATM dysfunction and inflammatory traits during obesity
• Identification of transcriptional differences between ATMs from lean vs obese adipose
tissue at several key points during the development of obesity and insulin resistance
may reveal upstream triggers, regulatory factors and intracellular pathways that shape
ATM function
• Targeting metabolic capacity rather than the inflammatory phenotype of ATMs may
hold potential to restore ATM function and adipose tissue homeostasis in obese
individuals
21.
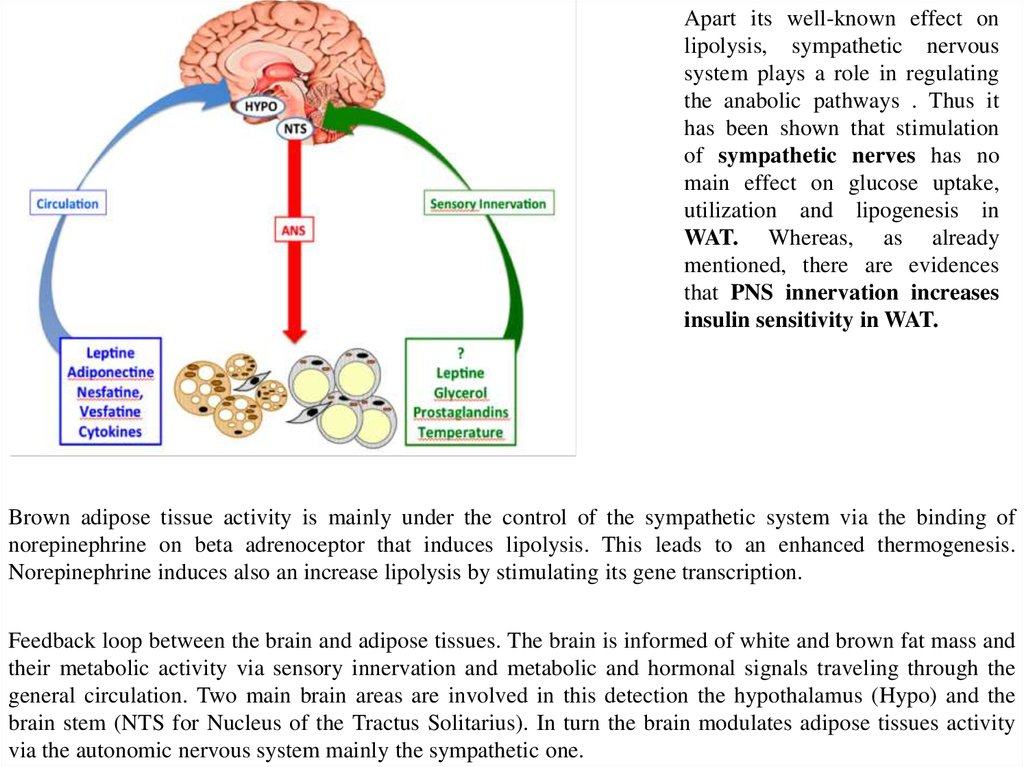
Apart its well-known effect onlipolysis, sympathetic nervous
system plays a role in regulating
the anabolic pathways . Thus it
has been shown that stimulation
of sympathetic nerves has no
main effect on glucose uptake,
utilization and lipogenesis in
WAT. Whereas, as already
mentioned, there are evidences
that PNS innervation increases
insulin sensitivity in WAT.
Brown adipose tissue activity is mainly under the control of the sympathetic system via the binding of
norepinephrine on beta adrenoceptor that induces lipolysis. This leads to an enhanced thermogenesis.
Norepinephrine induces also an increase lipolysis by stimulating its gene transcription.
Feedback loop between the brain and adipose tissues. The brain is informed of white and brown fat mass and
their metabolic activity via sensory innervation and metabolic and hormonal signals traveling through the
general circulation. Two main brain areas are involved in this detection the hypothalamus (Hypo) and the
brain stem (NTS for Nucleus of the Tractus Solitarius). In turn the brain modulates adipose tissues activity
via the autonomic nervous system mainly the sympathetic one.
22.
While it has long been clear that undernutrition can impair immunocompetence, more recently, theprogression of obesity has also been attributed to a shift in immune function from an M2 to M1 type
responses.
Work by both Spiegelman and Lumengetal demonstrate critical interactions between adipose tissue
metabolism and the immune system, and the active role of adipose tissue macrophage (ATM)
polarization in the progression of obesity. Lean individuals in a non-inflammatory state maintain a
relatively low percentage (~10–15%) of resident ATMs. Healthy adipose tissue consists of uniformly
distributed alternatively activated M2 macrophages. The M2 polarized state in healthy adipose tissue is
maintained by eosinophils, which secrete IL-4. Polarized M2 ATMs secrete interleukin-10 (IL-10),
which regulates glucose homeostasis within adipose tissue and systemic tissues including muscle. In
turn adipose resident invariant natural killer Tcells (iNKT) induces the M2 phenotype through
secretion of
IL-10. Healthy adipocytes, in turn, secrete anti-inflammatory adipokines such as
adiponectin, a hormone that acts synergistically with IL-4 to exert anti-inflammatory effects.
23.
The intimate interaction between adipocytes and ATMs (adipose tissue macrophages) mayreflect a common origin of these two cell types. Studies have shown not only cross-talk
between ATMs and adipocytes, but a great deal of plasticity between these two lineages
compartments. Furthermore, while still controversial several studies have suggested that some
adipocytes and adipose progenitors may be hematopoietic stem cell-derived. In addition,
Coussin et al.(2013) have shown that hematopoietic stem cells that can reconstitute lethally
irradiated recipient mice exist within adipose tissue, and more recent studies have supported the
concept that adipose tissue is an extramedullary source of hematopoietic stem/progenitor cells.
Yet other studies have demonstrated the phagocytic capacity of pre-adipocytes and adipocytes
suggesting they can adopt macrophage-like functions.
In the late 2000s, Lumeng et al. identified adipose tissue inflammation as an
important early event in the development of obesity related complications.
24.
In healthy adipose tissue, tissue remodeling is accompanied byangiogenesis to maintain oxygen supply and critical nutrients to
promote adipose tissue homeostasis. However, under pathological
conditions, the existing adipocytes enlarge, angiogenesis is limited,
and tissue hypoxia ensues, resulting in the recruitment of
inflammatory cells.
25.
26.
27.
28.
a | Adipocytes and nerve cells. Parenchymal sympathetic nerve fibres secretecatecholamines to regulate the development and the thermogenic function of brown and
beige adipocytes. Conversely, brown beige adipocytes might also promote nerve
remodelling by producing neurotrophic factors, including nerve growth factor (NGF), brainderived neurotrophic factor (BDNF) and neuregulin 4 (NRG4).
b | Brown and/or beige adipocytes and vasculature. Adipocytes secrete vascular
endothelial growth factor (VEGF) to stimulate angiogenesis. The enhanced vasculature
provides increased nutrition and oxygen to sustain thermogenesis in brown and beige
adipocytes, thereby promoting energy expenditure and insulin sensitivity.
c | Immune cell regulation of beige adipocytes. Interleukin-33 (IL-33) (of unknown
cellular source) activates group 2 innate lymphoid cells (ILC2s), which secrete IL-13 and
IL-5. IL-5 activates eosinophils, which produce IL-4. IL-4, in turn, induces the
differentiation of M2 macrophages, which provide a crucial source of catecholamines for
beige fat activation. IL-4 (from eosinophils or ILC2s) also acts directly on platelet-derived
growth factor receptor-α (PDGFRA)+ precursors to increase their proliferation and
differentiation into beige adipocytes. Furthermore, ILC2s secrete Met-encephalin peptides
to promote beige adipocyte differentiation. Meteorin-like protein (METRNL) secreted by
muscle and WAT activates eosinophils and type II cytokine signalling to drive beige
adipocyte development.
29.
Obesity increases the risk of developing a number ofserious health conditions, including:
1. Coronary heart disease
2. High blood pressure
3. Stroke
4. Type 2 diabetes
5. Cancer
6. Sleep apnea (внезапная остановка дыхания во сне)
7. Gallstones (желчный камень)
8. Osteoarthritis