
















































 Медицина
МедицинаПохожие презентации:










Pharmacology. Lecture 1
1. Pharmacology. lecture 1
Associate-professor Goldobina Galina2.
Medical pharmacology is the science of chemicals(drugs) that interact with the human body. These
interactions are divided into two classes:
Pharmacodynamics denotes the actions of the drug on
the body, such as mechanism of action and therapeutic
and toxic effects.
Pharmacokinetics describes the effects of the body on
drugs, eg, absorption, distribution, metabolism and
excretion.
3. Routes of administration: ADVANTAGES and DISADVANTAGES
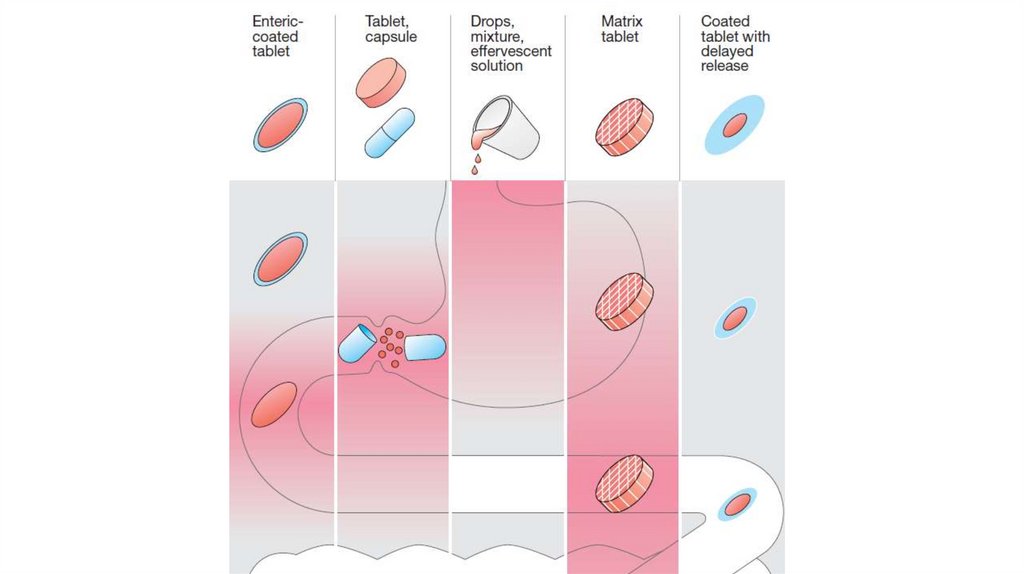
• Oral: the most common and safest, convenient, and economicalroute of administration, but absorption is affected by many
factors (food, HCl), drugs may be metabolized before systemic
absorption (first-pass effect). Patient compliance is necessary
• Sublingual: bypasses first-pass effect, destruction by stomach
acid, may cause immediate pharmacological effects, but limited
to certain types of drugs, to drugs that can be taken in small
doses, may loose part of the drug dose if it is swallowed
4.
5.
• Rectal: partially bypasses firstpass effect, destruction by stomachacid, ideal if drug causes vomiting,
in patients who are vomiting, or
comatose, but drugs may irritate
the rectal mucosa, not a wellaccepted route
6.
• Intravenous: can have immediate effects, ideal if dosed inlarge volumes, suitable for irritating substances and
complex mixtures, valuable in emergency situations,
dosage titration permissible, ideal for high molecular
weight proteins and peptide drugs, but unsuitable for oily
substances, may result in adverse effects, most substances
must be slowly injected, strict aseptic techniques are
needed
7.
• Subcutaneous: suitable for slow-release drugs, ideal forsome poorly soluble suspensions, but pain or necrosis if
drug is irritating, unsuitable for drugs administered in large
volumes
• Intramuscular: suitable if drug volume is moderate,
suitable for oily solutions and certain irritating substances,
preferable to intravenous if patient must self-administer, but
can be painful, can cause intramuscular hemorrhage
(precluded during anticoagulation therapy)
8.
9.
• Transdermal (patch): bypasses the first-pass effect,convenient and painless,
• ideal for drugs that are lipophilic and have poor oral
bioavailability,
• ideal for drugs that are quickly eliminated from the body,
• but some patients are allergic to patches, which can cause
irritation,
• drug must be highly lipophilic, may cause delayed delivery
of drug to pharmacological site of action,
• limited to drugs that can be taken in small daily doses.
10.
11.
• Inhalation: absorption is rapid; can have immediateeffects, ideal for gases,
• effective for patients with respiratory problems, dose can
be titrated, localized effect to target lungs: lower doses are
used compared to that with oral or parenteral
administration, fewer systemic side effects,
• But drug can enter the brain quickly, patient may have
difficulty regulating dose, some patients may have
difficulty using inhalers.
12.
13. Mechanisms of absorption of drugs
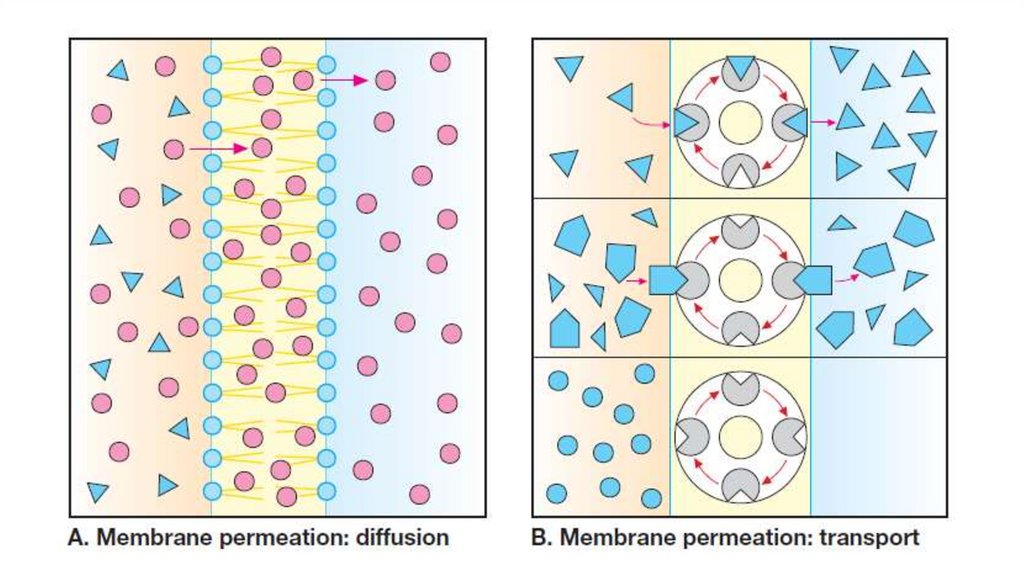
• Drugs may be absorbed from the GI tract by passive diffusion,filtration, facilitated diffusion, active transport, or pinocytosis.
• The driving force for passive absorption (filtration, passive
diffusion) of a drug is the concentration gradient across a
membrane separating two body compartments. The drug moves
from a region of high concentration to one of lower concentration.
• Filtration: water-soluble drugs penetrate the cell membrane
through aqueous channels or pores.
14.
• Diffusion: lipid-soluble drugs readily move across mostbiologic membranes due to their solubility in the membrane
lipid bilayers. Passive diffusion does not involve a carrier, is not
saturable, and shows a low structural specificity. The vast
majority of drugs are absorbed by this mechanism.
• Facilitated diffusion: agents can enter the cell through
specialized transmembrane carrier proteins, moving them from
an area of high concentration to an area of low concentration. It
does not require energy, can be saturated, and may be inhibited
by compounds that compete for the carrier.
15.
• Active transport: Energy-dependent, involves specific carrierproteins. It is capable of moving drugs against a concentration
gradient. The process is saturable. Active transport systems are
selective and may be competitively inhibited by other
cotransported substances.
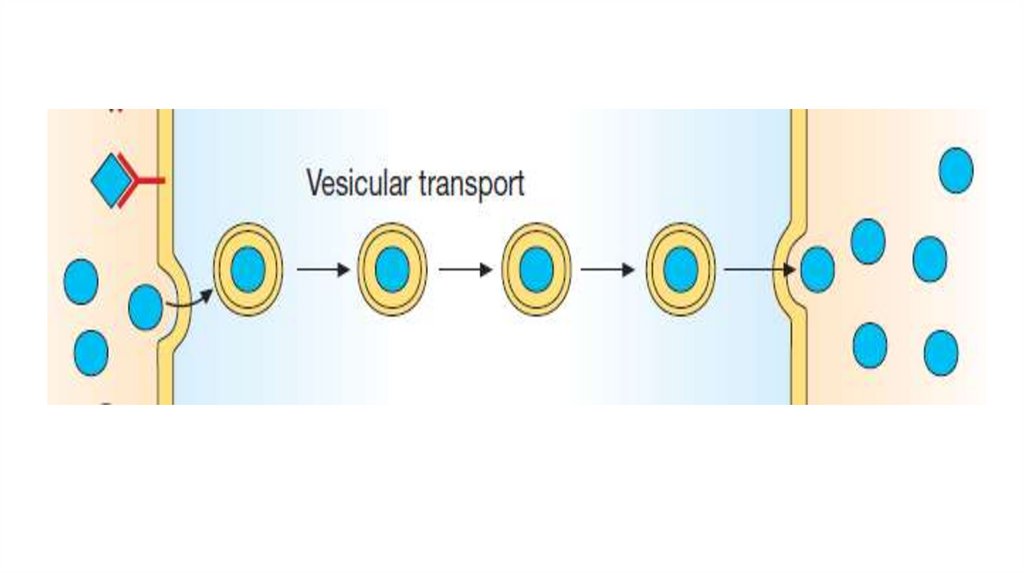
• Pinocitosis: This type of absorption is used to transport drugs of
exceptionally large size across the cell membrane. It involves
engulfment of a drug by the cell membrane and transport into the
cell by pinching off the drugfilled vesicle.
16.
17.
18. Bioavailability
• Bioavailability is the rate and extent to which anadministered drug reaches the systemic circulation.
For example, if 100 mg of a drug is administered
orally and 70 mg is absorbed unchanged, the
bioavailability is 0.7 or 70%. Determining
bioavailability is important for calculating drug
dosages
for
nonintravenous
routes
of
administration.
19.
• Determination of bioavailability: Bioavailability isdetermined by comparing plasma levels of a drug after a
particular route of administration (for example, oral
administration) with levels achieved by IV
administration. After IV administration, 100% of the
drug rapidly enters the circulation. When the drug is
given orally, only part of the administered dose appears
in the plasma.
• AUC - area under the curve.
F= AUCper os/ AUC iv х 100%
20.
21. Factors that influence bioavailability
• First-pass hepatic metabolism: When a drug isabsorbed from the GI tract, it enters the portal
circulation before entering the systemic circulation. If
the drug is rapidly metabolized in the liver or gut wall
during this initial passage, the amount of unchanged
drug entering the systemic circulation is decreased.
• Solubility of the drug: For a drug to be readily
absorbed, it must be largely lipophilic.
22.
• Chemical instability.• Nature of the drug formulation (salt form, crystal
polymorphism, enteric coatings, and the presence of
excipients: such as binders and dispersing agents).
23. Drug distribution
• Drug distribution is the process by which a drug reversiblyleaves the bloodstream and enters the interstitium
(extracellular fluid) and the tissues.
The distribution of a drug from the plasma to the
interstitium depends on:
• cardiac output and local blood flow,
• capillary permeability, the tissue volume,
• the degree of binding of the drug to plasma and tissue
proteins,
• and the relative lipophilicity of the drug.
24.
• Lipid-soluble drugs readily penetrate the CNS because theydissolve in the endothelial cell membrane. Ionized or polar
drugs generally fail to enter the CNS because they cannot
pass through the endothelial cells that have no slit junctions.
• The apparent volume of distribution, Vd, is defined as
the fluid volume that is required to contain the entire
drug in the body at the same concentration measured
in the plasma.
25.
26.
27. Elimination
• Once a drug enters the body, the process of eliminationbegins. The three major routes of elimination are hepatic
metabolism, biliary elimination, and urinary elimination.
• Renal elimination of a drug via the kidneys into urine
involves the processes of glomerular filtration, active
tubular secretion, and passive tubular reabsorption.
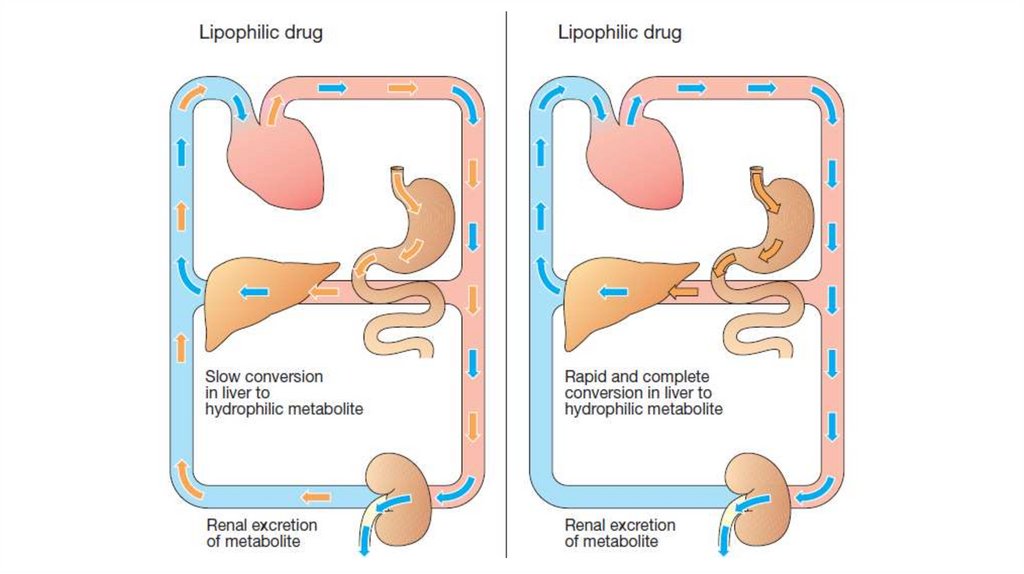
• The kidney cannot efficiently eliminate lipophilic drugs
that readily cross cell membranes and are reabsorbed in the
distal convoluted tubules.
28.
29.
• Metabolism in the liver leads to production of products withincreased polarity, which allows the drug to be eliminated.
• There are two general sets of reactions, called phase I and
phase II
• Phase I: reactions utilizing the P450 system convert
lipophilic drugs into more polar molecules. Phase I
reactions usually involve reduction, oxidation, or hydrolysis.
Phase I metabolism may increase, decrease, or have no effect
on pharmacologic activity.
30.
31.
• The CYP450-dependent enzymes are an important targetfor pharmacokinetic drug interactions.
• Inducers (for example, phenobarbital, rifampin, and
carbamazepine) are capable of increasing the synthesis of
one or more enzymes.
• The more important CYP inhibitors are erythromycin,
ketoconazole, because they each inhibit several enzymes.
32.
• Phase II: This phase consists of conjugation reactionswith an endogenous substrate, such as glucuronic acid,
sulfuric acid, acetic acid, or an amino acid, results in polar,
usually more water-soluble compounds that are often
therapeutically inactive. But morphine-6-glucuronide,
which is more potent than morphine. Glucuronidation is the
most common and the most important conjugation reaction.
• The highly polar drug conjugates are then excreted by the
kidneys or in bile.
33.
• Drug clearance may also occur via the intestines, bile,lungs, and breast milk, among others. Drugs that are not
absorbed after oral administration or drugs that are
secreted directly into the intestines or into bile are
eliminated in the feces. The lungs are primarily involved
in the elimination of anesthetic gases.
• Clearance (CL) estimates the amount of drug cleared
from the body per unit of time.
• Total CL reflects all mechanisms of drug elimination.
34. Pharmacodynamics. Effects
• Local effect occurs at the site of drug’s application .• Resorptive (systemic) effect develops after absorption of the
drug into the blood.
• Direct effect occurs at the site of contact of the drug with the
tissue.
• Reflect effect is produced when substances influence exteroor interoceptors causing changes in the status of nerve
centres or effector organs.
35. Drugs “’targets
• Few drugs (e.g. activated charcoal, osmoticdiuretics) act by virtue of their physicochemical
properties, and this is called non‐specific drug
action.
• Some drugs act as false substrates or inhibitors for
certain transport systems or enzymes.
36.
• Enzymes. Drugs that act by inhibiting enzymesinclude:
• anticholinesterases, which enhance the action of
acetylcholine;
• carbonic anhydrase inhibitors, which are diuretics
(i.e. increase urine flow);
• monoamine
oxidase
inhibitors,
which
are
antidepressants;
• and inhibitors of cyclooxygenase (NSAIDs) .
37.
• Drugs can influence on ion channels (selective poresin the membrane).
Among drugs affecting ion channels there are local
anesthetics, antiarhythmic, antiepileptic drugs.
38.
• However, most drugs produce their effects byacting on specific proteins. These proteins are
called receptors, and they normally respond to
endogenous chemicals in the body. These
chemicals are either synaptic transmitter
substances
or hormones. For example,
acetylcholine is a transmitter substance released
from motor nerve endings.
39.
• A receptor as any biologic molecule to which a drug bindsand produces a measurable response. The receptors may be
divided into four families:
1) ligand-gated ion channels (nicotinic receptor,
γ‐aminobutyric acid (GABA) receptor),
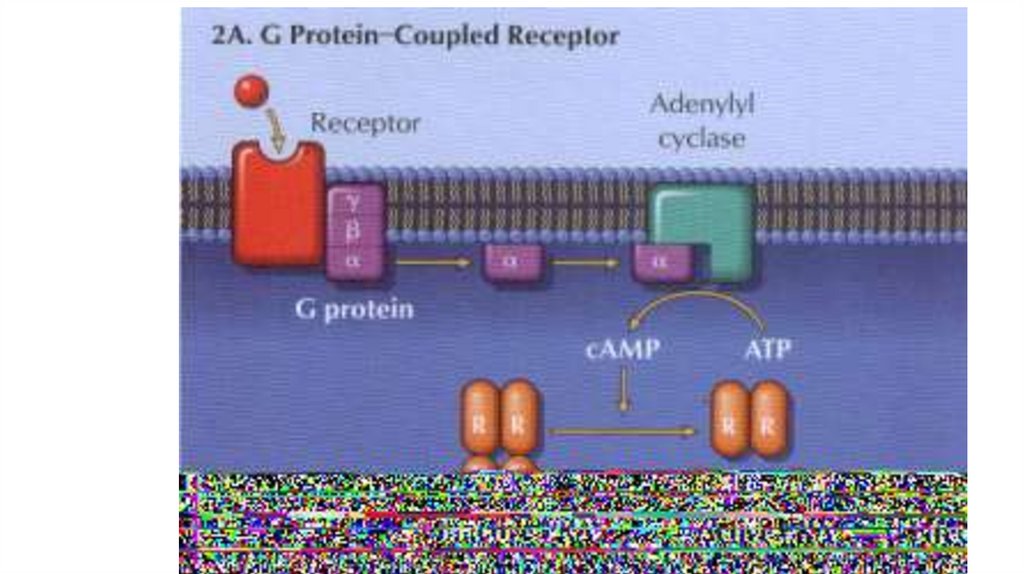
2) G protein–coupled receptors,
40.
41.
42.
3) Kinase‐linked receptors are surface receptorsthat possess (usually) intrinsic tyrosine kinase
activity. They include receptors for insulin,
cytokines and growth factors.
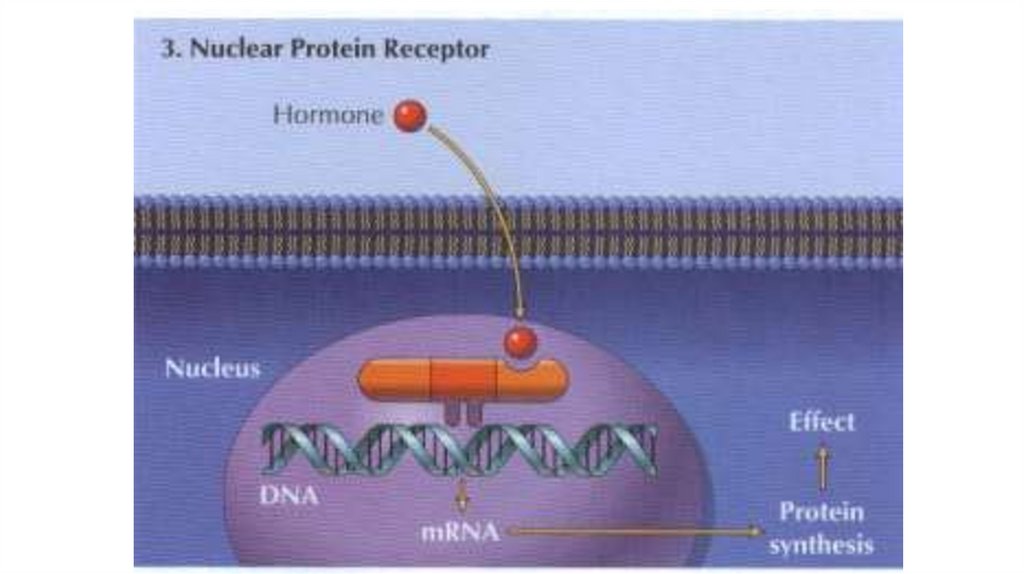
4) Nuclear receptors for steroid hormones and
thyroid hormones are present in the cell nucleus
and regulate transcription and thus protein
synthesis.
43.
44.
45.
• Chemicals (e.g. acetylcholine) or drugs that activatereceptors and produce a response are called agonists .
• Affinity is a measure of how avidly a drug binds to its
receptor.
• Intrinsic efficacy. This is the ability of an agonist to alter
the conformation of a receptor in such a way that it elicits a
response in the system.
• The interaction between a drug and the binding site of the
receptor depends on the complementarity of ‘fit’ of the two
molecules.
46.
• Partial agonists. These are agonists that cannotelicit the same maximum response as a ‘full’
agonist.
• Some drugs, called antagonists, combine with
receptors, but do not activate them. Antagonists
reduce the probability of the transmitter substance
(or another agonist) combining with the receptor
and so reduce or block its action.
47.
48.
49.
• The durability of the “Drug-receptor” bond determineswhether the drug action is reversible (characteristic for
most drugs) or irreversible (in case of covalent bond).
• The ability of a drug to combine with one particular type
of receptor is called specificity. No drug is truly specific,
but many have a relatively selective action on one type
of receptor.
• Drugs are prescribed to produce a therapeutic effect, but
they often produce additional unwanted effects or side
(adverse effects) that range from the trivial (e.g. slight
nausea) to the fatal (e.g. aplastic anaemia).
50.
Potency is a measure of the amount of drug necessary toproduce an effect of a given magnitude. The dose of drug
producing 50% of the maximum effect (ED50) is usually used
to determine potency.
51.
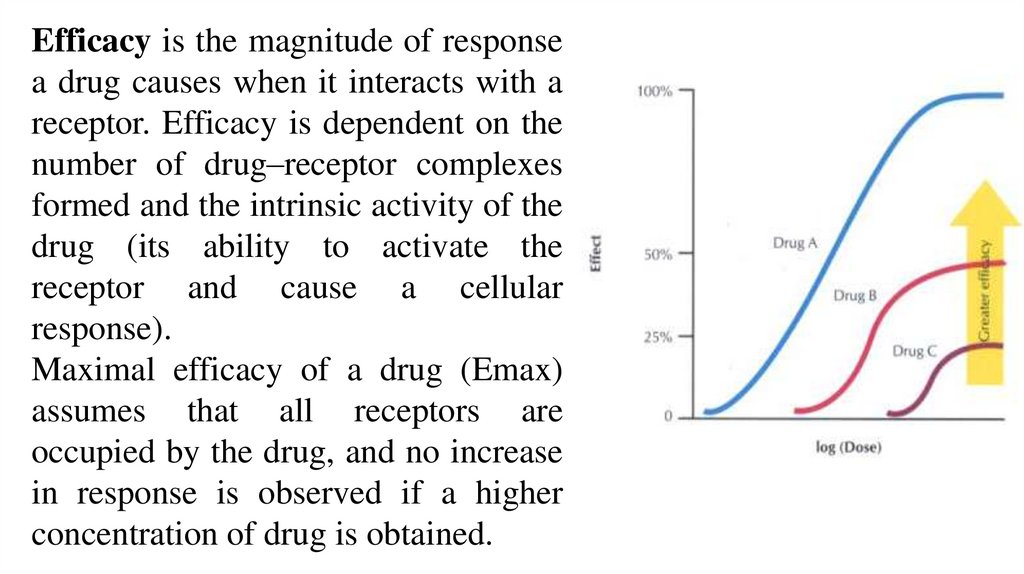
Efficacy is the magnitude of responsea drug causes when it interacts with a
receptor. Efficacy is dependent on the
number of drug–receptor complexes
formed and the intrinsic activity of the
drug (its ability to activate the
receptor and cause a cellular
response).
Maximal efficacy of a drug (Emax)
assumes that all receptors are
occupied by the drug, and no increase
in response is observed if a higher
concentration of drug is obtained.
52. Drugs interactions
• Pharmacokinetic• Pharmacodynamic:
A.Synergism
B.Antagonism
53.
• In case of synergism drug interaction leads to anincrease in effect. Synergism may be direct (if both
compounds affect one substrate) or indirect (if their
effects have different localization).
• Diuretics enhance the effect of angiotensin-converting
enzyme inhibitors in the treatment of hypertension
(indirect).
• Paracetamol enhances the effect of metamizole (direct).
• Drugs with similar actions, e.g. benzodiazepines and
alcohol, produce additive effects and may cause severe
central nervous system depression.
54. Interaction of drugs Synergism
Summation(paracetamol + metamizol
sodium)
1
1
2
Potentiation
(paracetamol +
diphenhydramine))
1
1
3
55.
Antagonism
The ability of a drug to decrease the effect of the other one is called
antagonism. It may be direct or indirect also.
Conversely, drugs may have opposite actions, e.g. in asthmatic
patients β‐blockers will oppose β‐agonists and may precipitate
severe or even fatal asthma.
Most antagonists are drugs that bind to receptors but do not activate
them. They may be competitive or irreversible. Other types of
antagonist are less common.
Competitive antagonists bind reversibly with receptors, and the
tissue response can be returned to normal by increasing the dose of
agonist.
56.
• Irreversible antagonists have an effect that cannot be reversedby increasing the concentration of agonist. The only important
example is phenoxybenzamine, which binds covalently with
α‐adrenoceptors.
• Non‐competitive antagonists do not bind to the receptor site but
act downstream to prevent the response to an agonist, e.g.
calcium‐channel blockers.
• Chemical antagonists simply bind to the active drug and
inactivate it; e.g. protamine abolishes the anticoagulant effect of
heparin.
• Physiological antagonists are two agents with opposite effects
e.g. prostacyclin and thromboxane A2 on platelet aggregation.
57.
• Synergoantagonism occurs when some effects of thecombined drugs are intensified and others are weakened.
For example, α-adrenoblockers lead to a decrease in
epinephrine stimulation of vessels α-adrenoreceptors, but its
effect on vessels β-adrenoreceptors becomes more marked.
58.
Pharmacokinetic interactions• Absorption. Drugs that increase (e.g. metoclopramide) or
decrease (e.g. atropine) the rate of gastric emptying may
affect absorption. Enterohepatic recirculation of oral
contraceptives (especially low‐dose oestrogen) may be
decreased by antibiotics and lead to pregnancy (antibiotics
kill the gut bacteria that normally release the steroid from
the conjugated form excreted in bile).
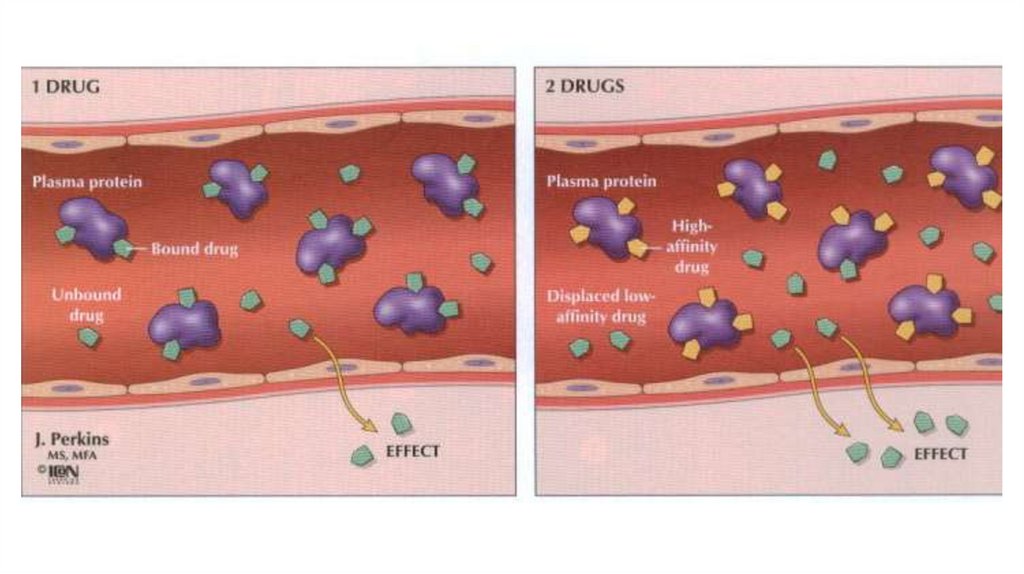
• Distribution. Many drugs are bound to plasma albumin and
may be displaced by a second drug.
59.
• Metabolism. Induction of hepatic enzymes by a second drug(e.g.phenobarbital, rifampicin) can decrease the efficacy of
drugs metabolized by the same enzymes (e.g.warfarin).
Enzyme inhibitors (e.g. cimetidine) potentiate the effects of
warfarin and may cause phenytoin and theophylline toxicity.
• Excretion. Drugs may share the same transport system in the
proximal tubules. Thus, probenecid competitively reduces
penicillin excretion. Potassium‐sparing diuretics combined
with angiotensinconverting enzyme (ACE) inhibitors cause
hyperkalaemia.
60. Adverse drug reactions
• Adverse drug reactions can be divided into those that arepredictable and dose‐related (e.g. hypoglycaemia with
insulin, bleeding with warfarin) or sometimes a drug’s
parallel unwanted action (e.g. respiratory depression with
morphine).
• and those that are unpredictable and not necessarily
dose‐related (drug allergy or immunological reactions,
idiosyncrasy).
61.
• Cumulation – storage of pharmacological substance inthe body. It is typical for slow-acting drugs, that are
released slowly or are steadily bound in the body.
Cumulation after repeated administration may be the
cause of toxic effects.
• Renal disease can lead to accumulation and toxicity
if a drug is excreted by glomerular filtration or tubular
secretion (e.g. gentamicin and other aminoglycosides,
digoxin, amphotericin, captopril). Liver disease can
lead to accumulation of drugs metabolized in the liver.
62.
Tachyphylaxis, desensitization, tolerance and drug resistanceWhen a drug is given repeatedly, its effects often decrease
with time. If the decrease in effect occurs quickly (minutes),
it is called tachyphylaxis or desensitization.
63.
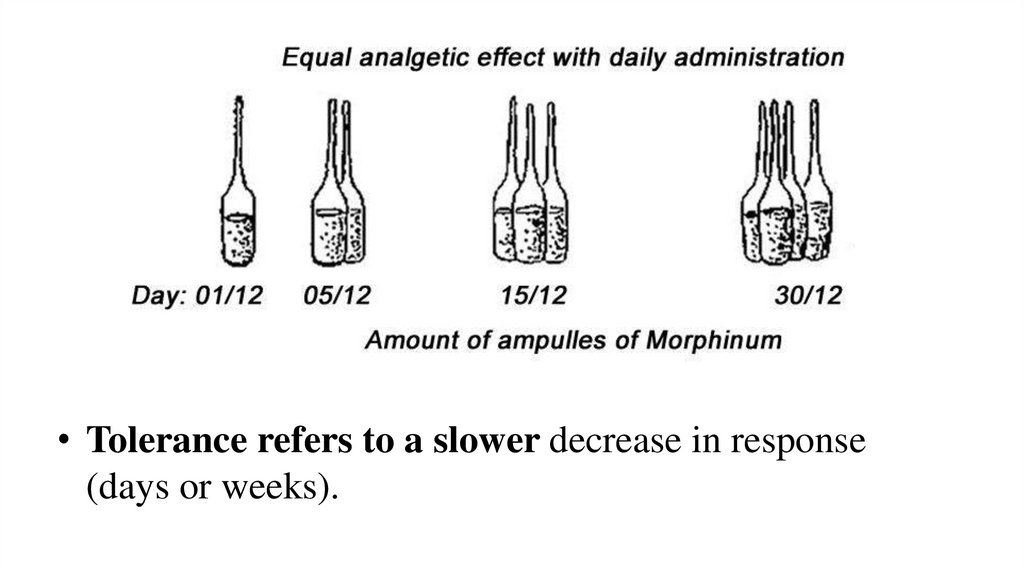
• Tolerance refers to a slower decrease in response(days or weeks).
64.
• Tolerance may involve increased metabolism of a drug,e.g. ethanol, barbiturates, or homeostatic mechanisms
(usually not understood) that gradually reduce the effect
of a drug, e.g. morphine. Changes in receptors may cause
desensitization, e.g. suxamethonium. . A decrease in
receptor number (downregulation) can lead to tolerance,
e.g. insulin.
• Drug resistance is a term reserved for the loss of effect
of chemotherapeutic agents, e.g. antimalarials.
65.
• Drug dependence is a term used when a person has acompulsion to take a drug in order to experience its psychic
effects, and sometimes to avoid the discomfort of withdrawal
symptoms.
• Psychological dependence: cocaine, LSD, psilocin. Cannabis
has hallucinogenic action. It produces feelings of euphoria,
relaxation and well‐being.
• Physical dependence on opioid analgesics gradually develops,
and sudden termination of drug administration precipitates a
withdrawal syndrome (characterized by yawning, sweating,
gooseflesh, tremor, irritability, anorexia, nausea and vomiting).
66.
• Teratogenesis is the occurrence of fetal developmentalabnormalities caused by drugs taken during the first
trimester of pregnancy. Most drugs cross the placental
barrier to some extent and, if possible, drugs should be
avoided during pregnancy.
• Known teratogens include alcohol (fetal alcohol syndrome),
anticancer drugs, warfarin (multiple congenital defects),
valproate, carbamazepine (neural tube defects), and other
anticonvulsants and tetracyclines (inhibition of bone
growth).
67.
68.
• Carcinogenesis. Drug‐induced tumours areprobably very rare because the pharmaceutical
industry makes great efforts to avoid marketing
carcinogenic agents. The mechanisms involved in
chemical carcinogenesis are usually unknown, but
immunosuppression (e.g. azathioprine with
prednisolone) is associated with a greatly increased
risk of lymphomas.
69. Literature
1. Tripathi K.D. Essentials of Medical Pharmacology. Eighth Edition. -2019.- Jaypee Brothers Medical Publishers. TheHealth Sciences Publisher. -New Delhi. London. Panama
2. D.A.Kharkevich. Pharmacology. Textbook for medical students. Translation of 12th edition of Russion textbook
“Pharmacology” (2017). – М., ГЭОТАР-Медиа, 2017.
3. Review of pharmacology. Gobind Rai Garg, Sparsh Gupta. 13th edition. - 2019.- Jaypee Brothers Medical Publishers.
The Health Sciences Publisher. -New Delhi. London. Panama
4. Whalen Karen. Lippincott Illustrated Reviews: Pharmacology. Sixth Edition. - Wolters Kluwer. - 2015.-Philadelphia
5. Color Atlas of Pharmacology. 2nd edition, revised and expanded. Heinz Lüllmann.- 2000 Thieme
6. Pharmacology Examination & Board Review. Tenth Edition. Trevor Anthony J., Katzung Bertram G., Kruidering-Hall
Marieke, Susan B. Masters. - a LANGE medical book. - 2013.-New York
7. Medical Pharmacology at a Glance. Eighth Edition. Neal Michael J. – 2016. John Wiley & Sons, Ltd.
8. USMLE Step 1. Lecture Notes. Pharmacology. Lionel P.Raymon and others.- Kaplan Medical.Inc. -2009