
 ACCOUNT FOR")















 Медицина
МедицинаПохожие презентации:










Optimizing surgical treatment of anterior cruciate ligament injuries
1. STATE EDUCATIONAL INSTITUTION "TAJIK STATE MEDICAL UNIVERSITY NAMED AFTER ABUALI IBNI SINO" DEPARTMENT OF TRAUMATOLOGY AND
2. RELEVANCE This topic is as follows ACCORDING TO THE LITERATURE, INJURIES TO THE ANTERIOR CRUCIATE LIGAMENT (ACL) ACCOUNT FOR
27-67.9% OF ALL INJURIES AND 33-92% OF INJURIESTO THE KNEE JOINT LIGAMENTS
(Michael A., 2011; Lind M., 2009; Orlyansky V., 2016)
3. PURPOSE OF THE STUDY • To improve the efficiency of ACL reconstruction. • To accelerate regeneration and improve functional
outcomes.• To study the role of SVF and PRP.
4. RESEARCH MATERIALS The paper analyzes the results of arthroscopic anterior cruciate ligament reconstruction surgery in 224
patients treated in the traumatology andorthopedics department of the state institution
"ISTIKLOL HEALTH COMPLEX" for the period
2021-2025.
5. Category patients
1. GenderA. Men - 221
B. Women - 3
2. Age
A. 17 to 30 years - 90
B. 30 to 45 years - 131
6. - Clinical symptoms - Ultrasound - Magnetic resonance imaging - Diagnostic arthroscopy
DIAGNOSTIC METHODS7.
Stages of patientpreparation for
surgery
8.
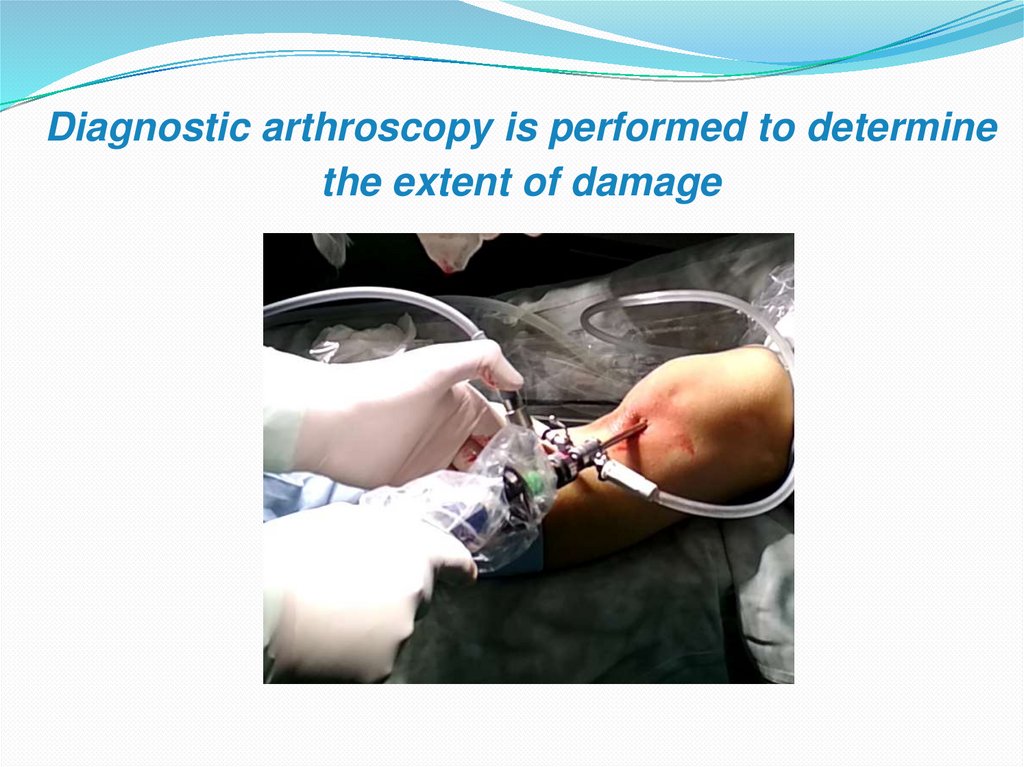
Diagnostic arthroscopy is performed to determinethe extent of damage
.
9.
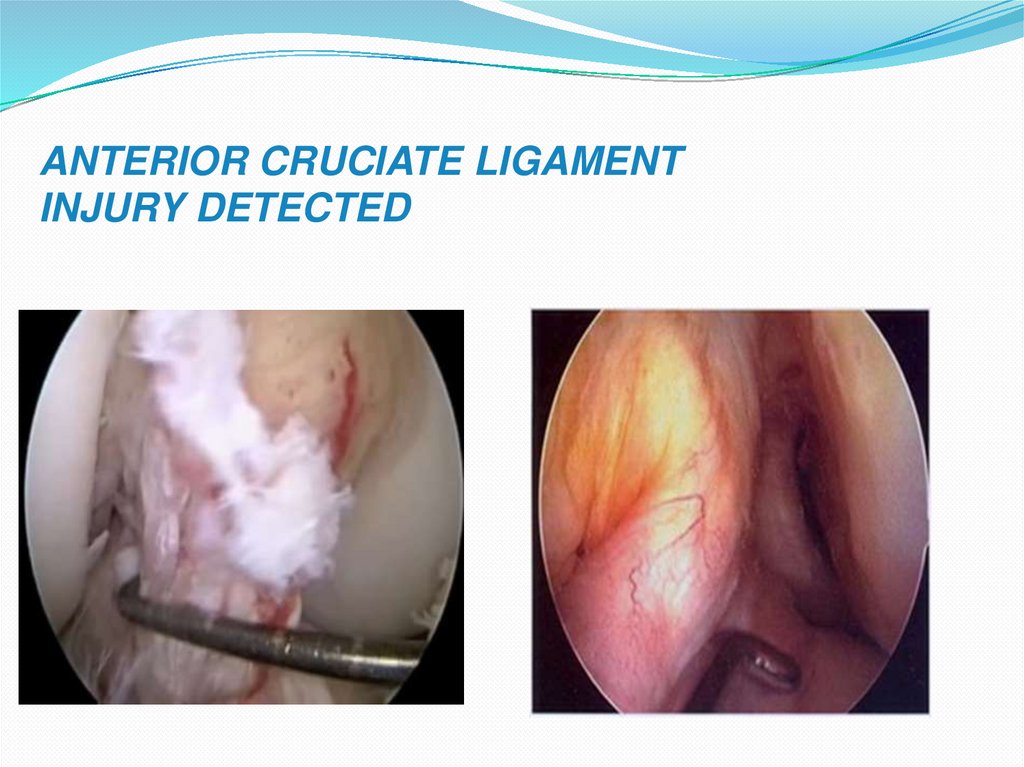
ANTERIOR CRUCIATE LIGAMENTINJURY DETECTED
10.
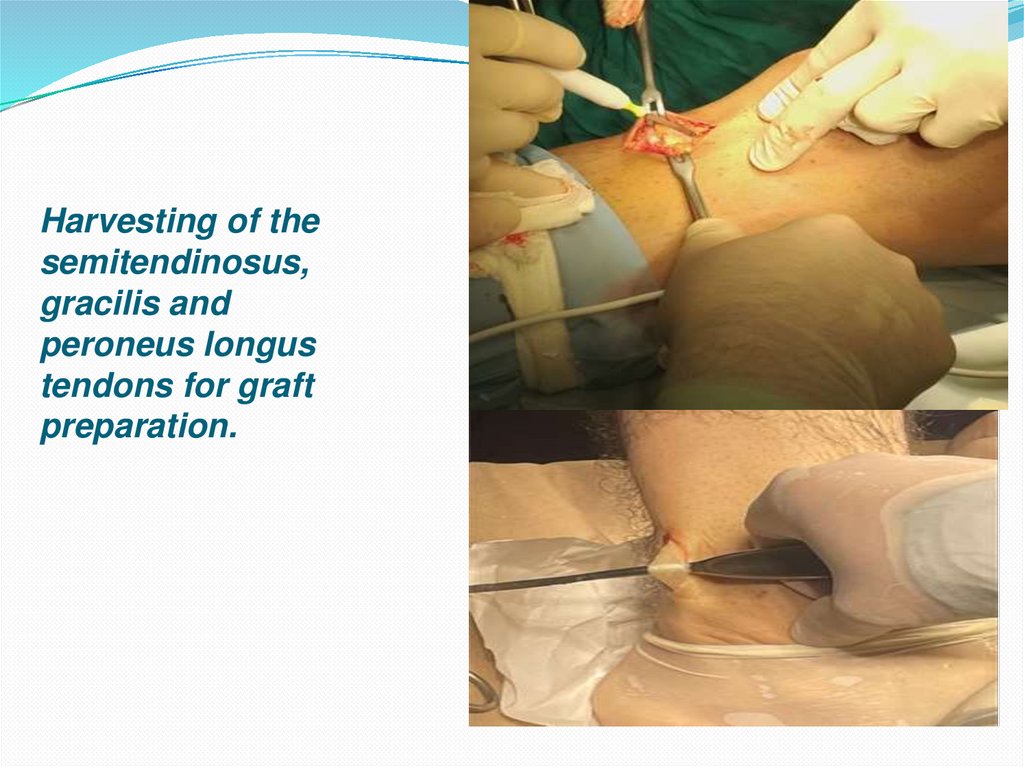
Harvesting of thesemitendinosus,
gracilis and
peroneus longus
tendons for graft
preparation.
11.
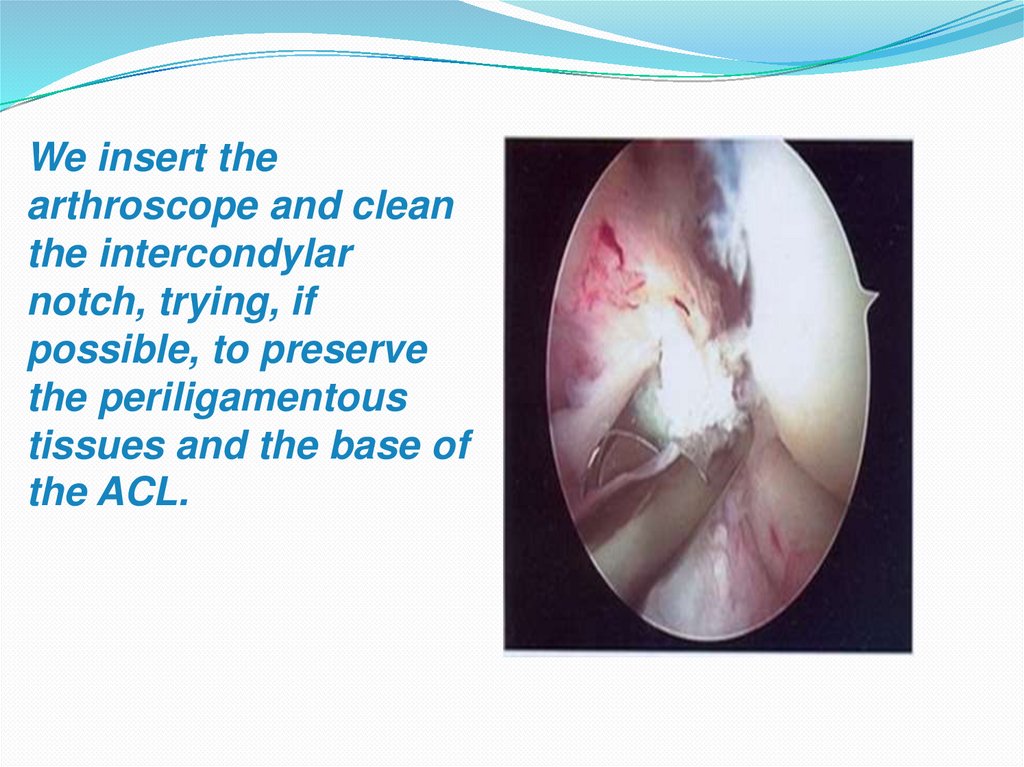
We insert thearthroscope and clean
the intercondylar
notch, trying, if
possible, to preserve
the periligamentous
tissues and the base of
the ACL.
12.
Stages of transplant preparation:muscle tissue is removed; tendons
are folded in half, sutured together
and fixed under tension.
13.
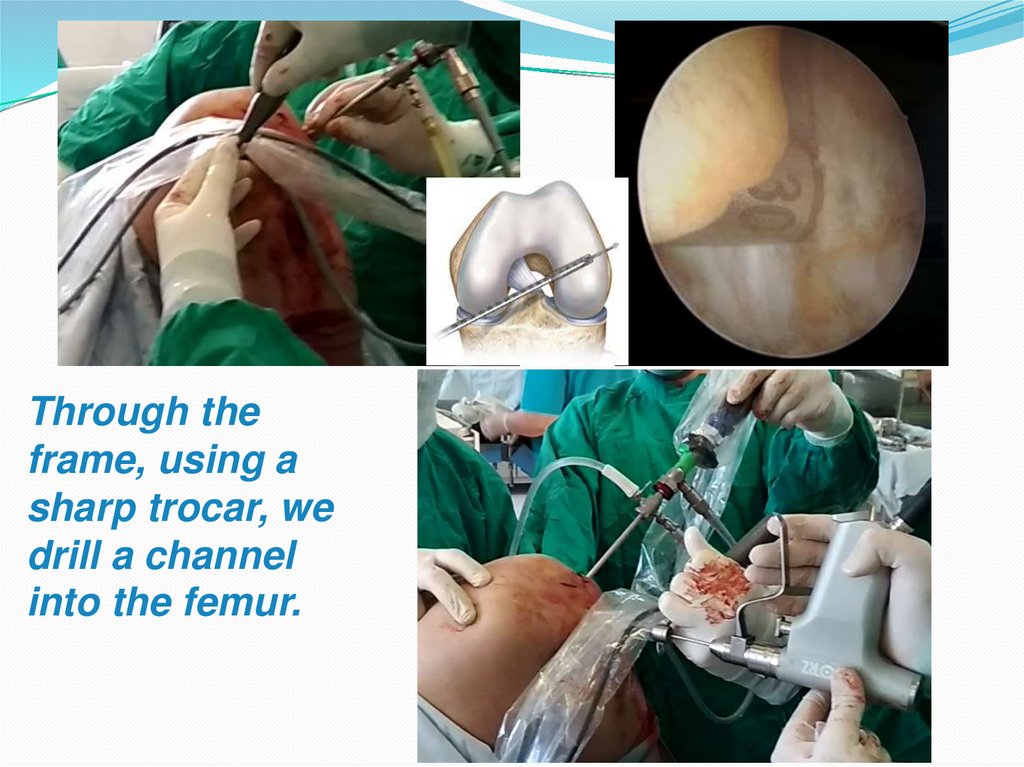
Through theframe, using a
sharp trocar, we
drill a channel
into the femur.
14.
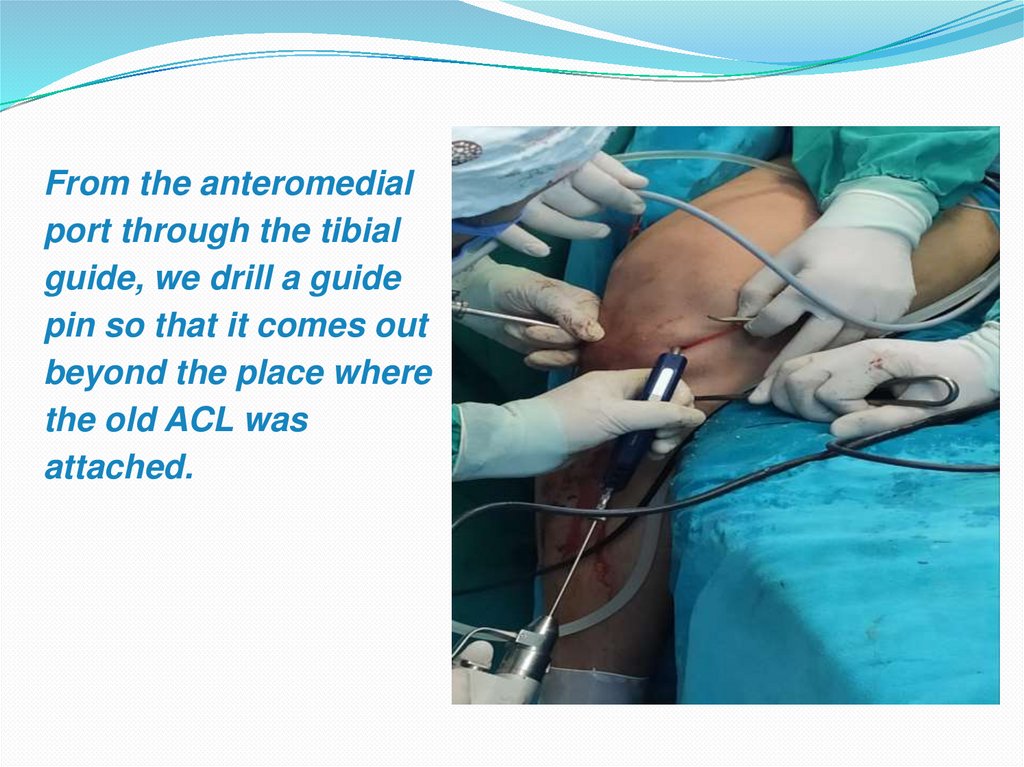
From the anteromedialport through the tibial
guide, we drill a guide
pin so that it comes out
beyond the place where
the old ACL was
attached.
15.
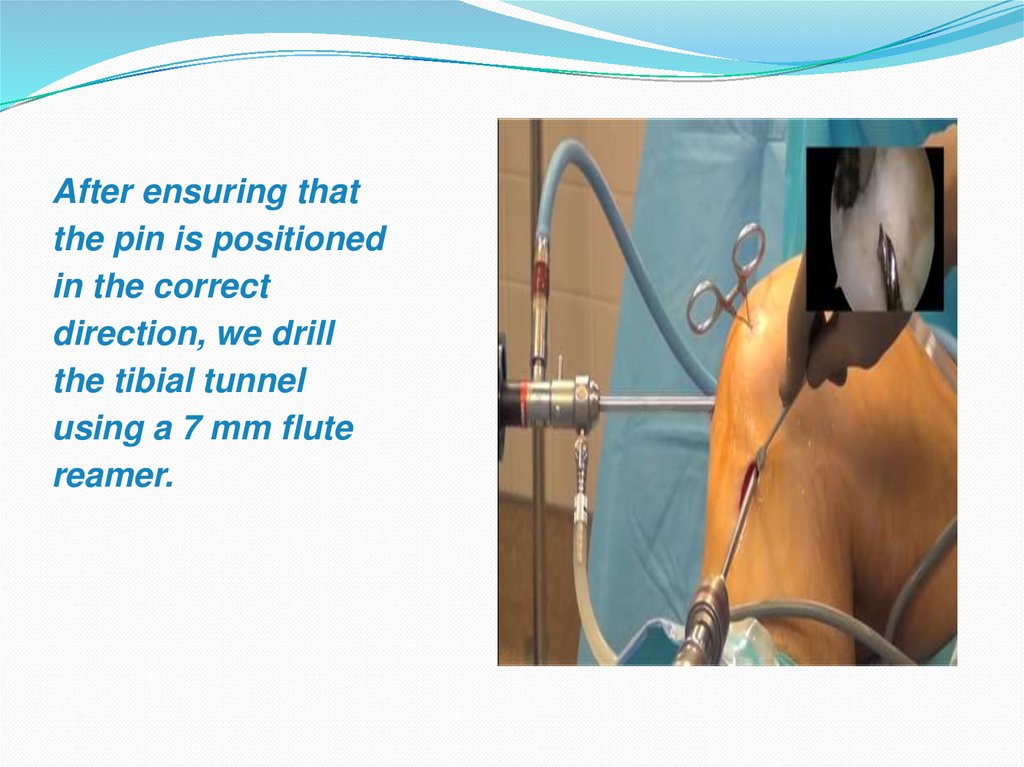
After ensuring thatthe pin is positioned
in the correct
direction, we drill
the tibial tunnel
using a 7 mm flute
reamer.
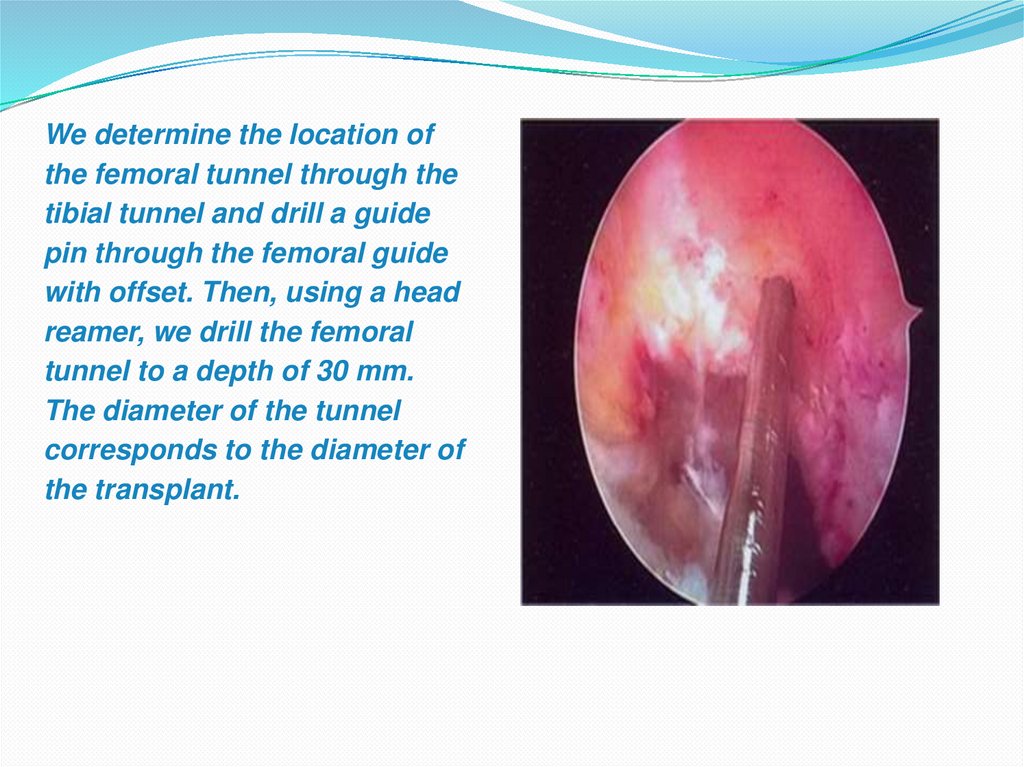
16.
We determine the location ofthe femoral tunnel through the
tibial tunnel and drill a guide
pin through the femoral guide
with offset. Then, using a head
reamer, we drill the femoral
tunnel to a depth of 30 mm.
The diameter of the tunnel
corresponds to the diameter of
the transplant.
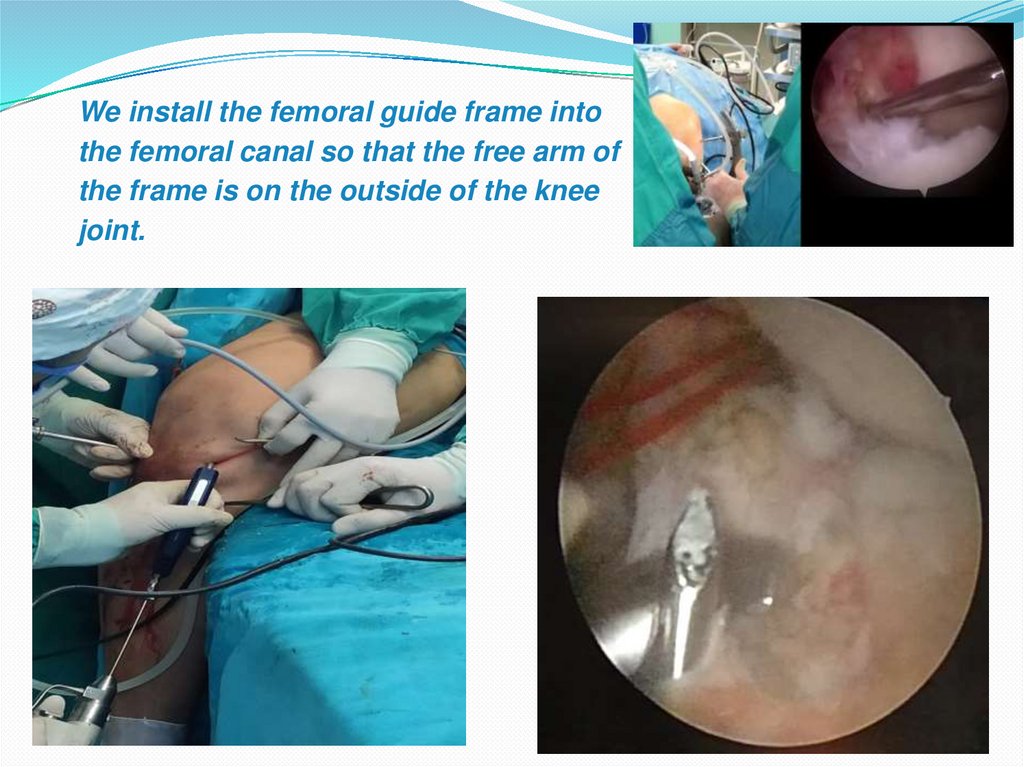
17.
We install the femoral guide frame intothe femoral canal so that the free arm of
the frame is on the outside of the knee
joint.
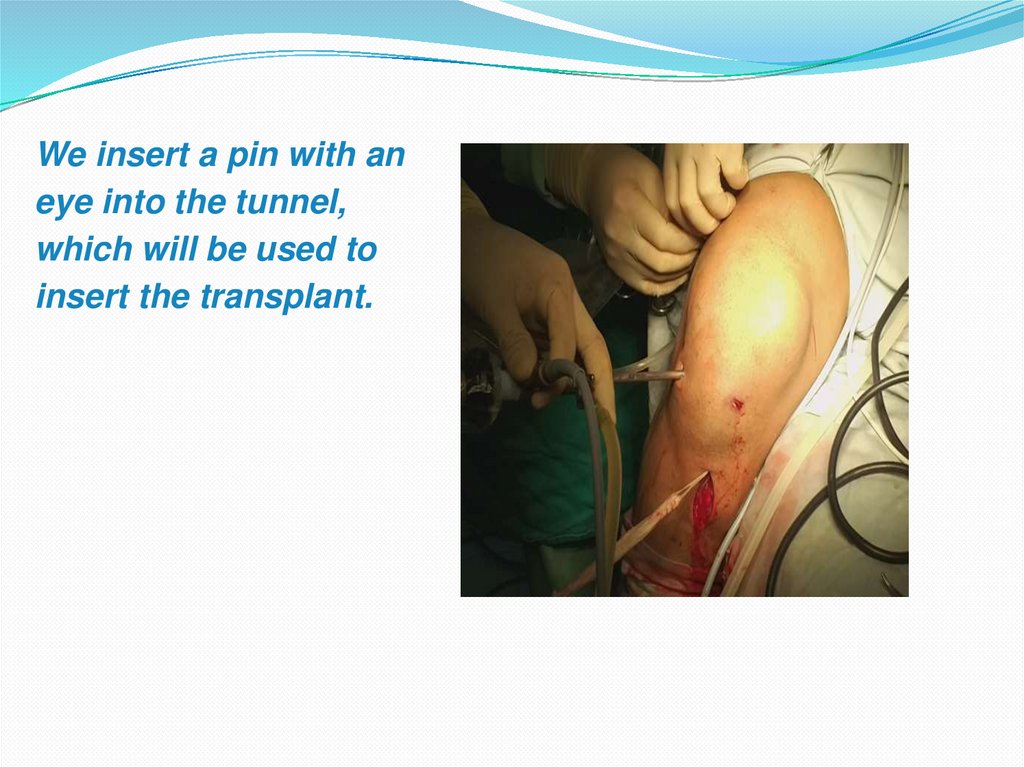
18.
We insert a pin with aneye into the tunnel,
which will be used to
insert the transplant.
19.
Under arthroscopecontrol, we introduce
the transplant into the
tunnel.
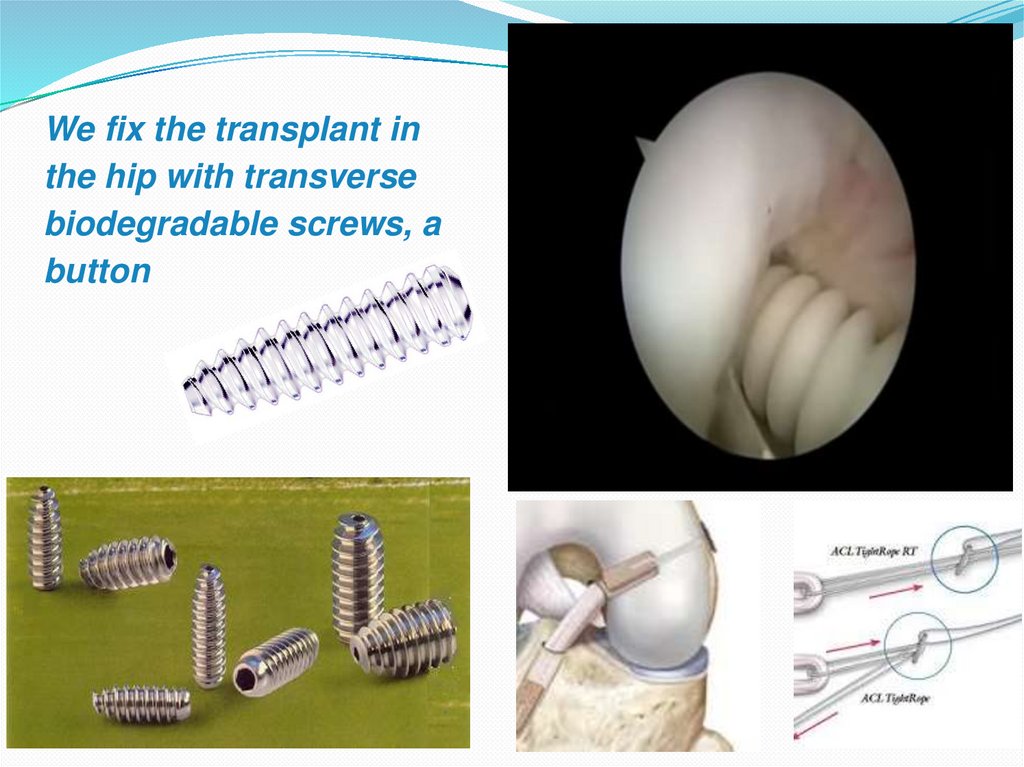
20.
We fix the transplant inthe hip with transverse
biodegradable screws, a
button
21. Fixation
Fixation on the thigh and lower leg:Titanium screw
Absorbable screws
Strength – 300-700 N
22.
The condition of the installed ACL graft ischecked
23. Application of PRP and SVF therapy for ACL injury
1. PRP: contains growth factors (PDGF, TGF-b, VEGF),which stimulate chondrocytes to recover. Injections are
made in courses of 2-4 procedures.
2. SVF (stromal-vascular fraction):
Obtained by lipoaspiration and then processed and
injected directly into the transplant and joint. These cells
have anti-inflammatory, angiogenic and
chondroprotective effects.
24. POSTOPERATIVE NTRODUCTION - the lower limb is immobilized by direct knee arthesis - analgesics and antibiotic therapy -
prevention of thromboembolic complications25. ASSESSMENT OF RESULTS USING THE LYSHALM SCALE
100%90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
double-literal
non-double-literal
good
26. TREATMENT RESULTS - long-term results of surgical treatment from 6 months to one year were studied in all operated patients -
good functional results were obtained in218 patients
- satisfactory treatment results were in 12
patients
27. Remote result after ACL plastic surgery:
28. CONCLUSION - AUTOGRAFTS FROM THE HOMOPLASTIC FLEXOR TENDONS AND THE LONG PERONEAL TENDON WITH THE USE OF PRP AND SVF THERAPY
CAN BE SUCCESSFULLY USED AS APLASTIC MATERIAL FOR ACL RECONSTRUCTION AND
ENHANCED REGENERATION
- THE USE OF THE GRAFT WILL PROVIDE A GOOD COSMETIC
MATERIAL AND DOES NOT INTERFERE WITH MOVEMENT IN
THE KNEE JOINT
- THE STRENGTH OF PRIMARY FIXATION AND THE
STRENGTH OF THE GRAFT ALLOWS TO START EARLY
REHABILITATION IN THE KNEE JOINT
29.
THANK YOU FORYOUR ATTENTION