







")

")


")
")
")
")









")
")












 Медицина
МедицинаПохожие презентации:



")





")
Myelodysplastic Syndromes
1. Myelodysplastic Syndromes
Dr. FinemanMYELODYSPLASTIC SYNDROMES
2. MDS
• Clonal stem cell disorders• Maturation defects
• Ineffective hematopoiesis
• Blood cytopenias
• Risk of transformation to AML
3. FEATURES USED TO DEFINE MDS
• Blood cytopenias• Ineffective hematopoiesis
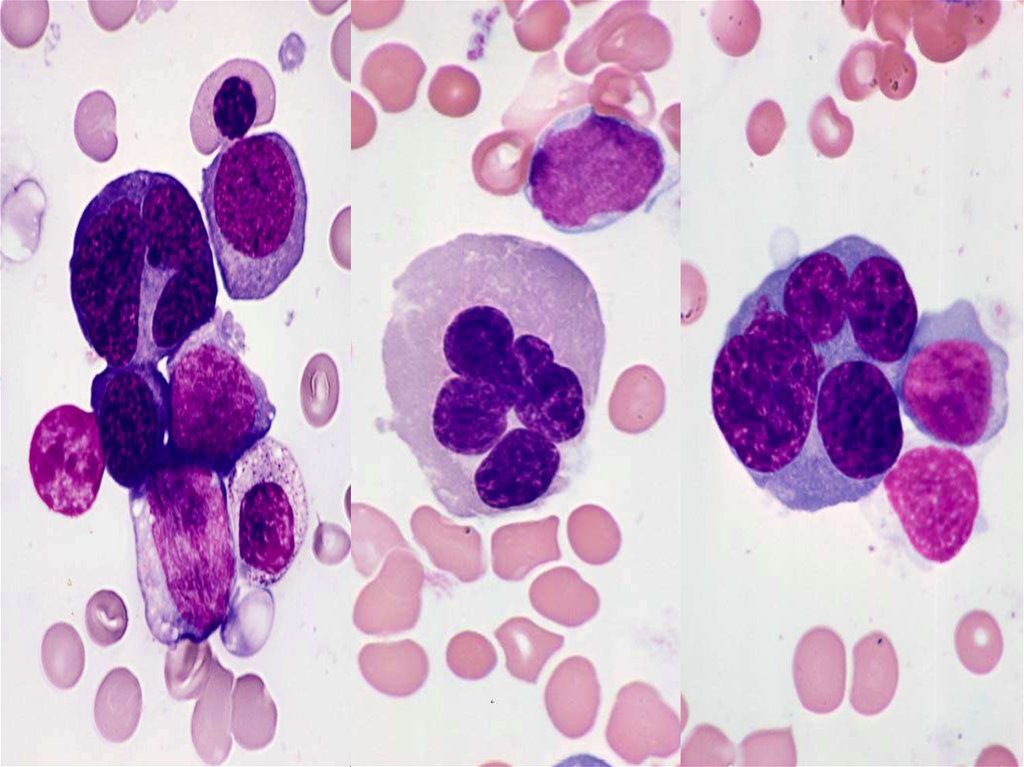
• Dyserythropoiesis
• Dysgranulopoiesis
• Dysmegakaryopoiesis
• Increased myeloblasts
4.
5.
6.
7. FAB CLASSIFICATION OF MDS
• Refractory Anemia• Refractory Anemia with Ringed Sideroblasts
• Refractory Anemia with Excess Blasts
(RAEB)
• Refractory Anemia with Excess Blasts in
Transformation (RAEB-T)
• Chronic Myelomonocytic Leukemia (CMML)
8. WHO CLASSIFICATION OF MDS
• Refractory anemia• Refractory anemia with ringed sideroblasts
• Refractory cytopenia with multilineage
dysplasia (RCMD) with or without ringed
sideroblasts
• Refractory anemia with excess blasts (RAEB)
• RAEB type 1 (5%-9% blasts)
• RAEB type 2 (10-19% blasts)
• MDS, unclassifiable
• MDS associated with isolated del (5q)
chromosome abnormality (“5q- syndrome”)
9. MAJOR CHANGES IN WHO CLASSIFICATION OF MDS
• Blast count for a diagnosis of AML isreduced from 30% to 20%
• RAEB-T is eliminated
• Refractory cytopenia with multilineage
dysplasia (RCMD) is added
• 5q- syndrome is added
• CMML is incorporated into a bridging MDSMPD classification
10. REFRACTORY ANEMIA (RA)
• Only erythroid lineage involved• Normocytic or macrocytic anemia
• Reticulocytopenia
• Usually normal or ↑RBC precursors
• Variable dyserythropoiesis
• <5% blasts in BM, none in blood
11.
12. REFRACTORY CYTOPENIA WITH MULTILINEAGE DYSPLASIA (RCMD)
• Usually bicytopenia or pancytopenia• Multilineage dysplasia
• <5% blasts in blood or BM
• May have ringed sideroblasts
• Worse prognosis than for RA and RARS and
a higher incidence of cytogenetic
abnormalities
13.
14.
15.
16. MDS WITH ISOLATED del(5q)
• Refractorymacrocytic
anemia
• Thrombocytosis
• Hypolobulated
megakaryocytes
• Stable clinical
course
17. REFRACTORY ANEMIA WITH EXCESS BLASTS (RAEB)
• Usually pancytopenia orbicytopenia
• Multilineage dysplasia
• 5% to 19% blasts in blood
or BM
• Type 1 - 5-9% blasts
• Type 2 - 10-19% blasts
• May have ringed
sideroblasts
• Absence of specific AML
cytogenetic abnormalities
18. REFRACTORY ANEMIA WITH EXCESS BLASTS (RAEB)
19. MYELODYSPLASTIC SYNDROME UNCLASSIFIABLE (MDS-U)
• Cytopenias• No or rare blasts in blood
• Unilineage dysplasia
• <5% marrow blasts
• No Auer rods
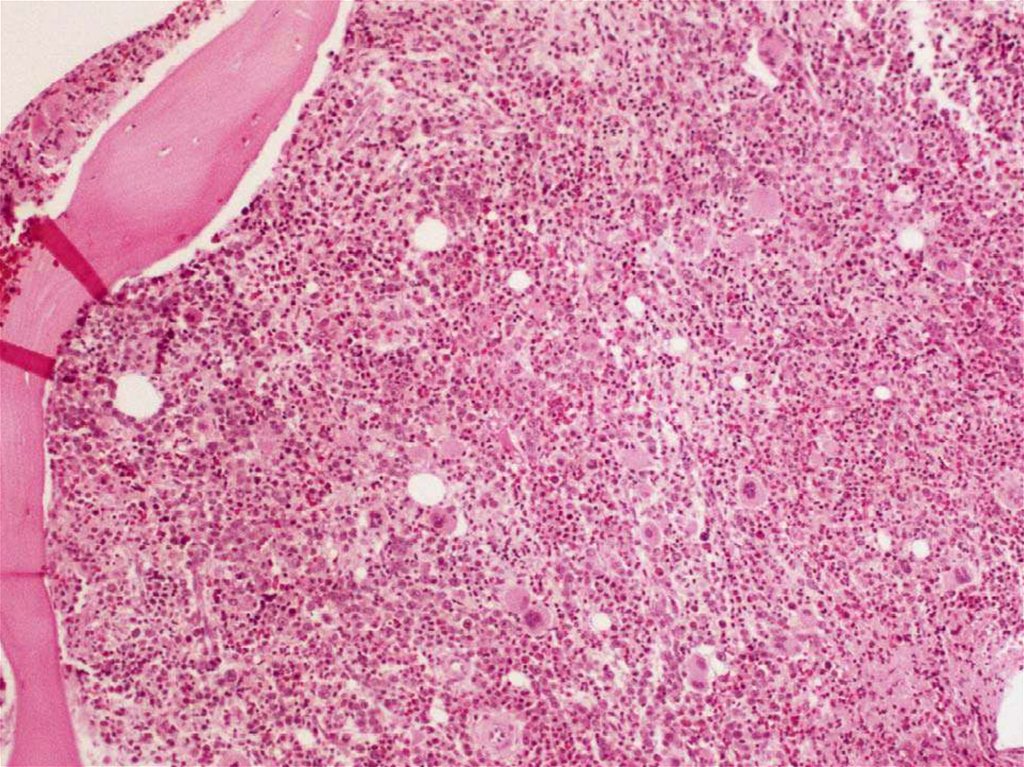
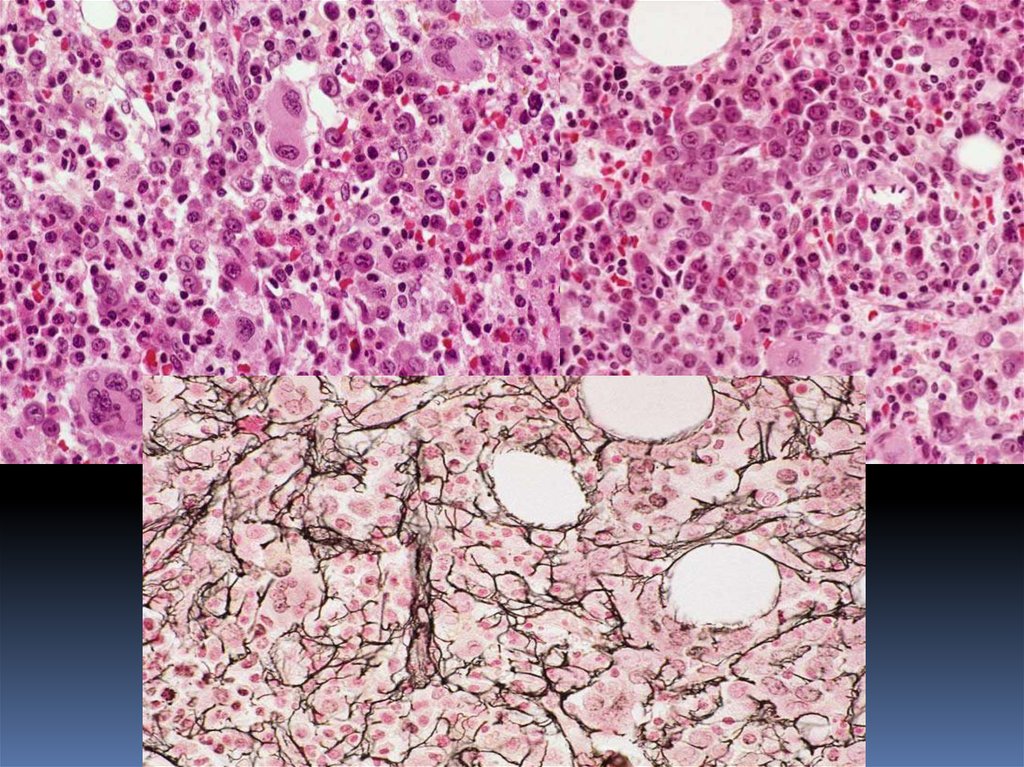
20. MYELODYSPLASTIC SYNDROME WITH INCREASED MARROW FIBROSIS
• Pancytopenia• Trilineage dysplasia
• Bone marrow fibrosis
• ↑and dysplastic megakaryocytes
• No splenomegaly
• ? poor survival
21.
22. HYPOCELLULAR MDS
• Cellularity of marrow<30%; (<20% in
patients over 60 yrs)
• ~ 10% of cases
• More common in
therapy related MDS
and in children with
MDS
• RA, RCMD, and RAEB
most common
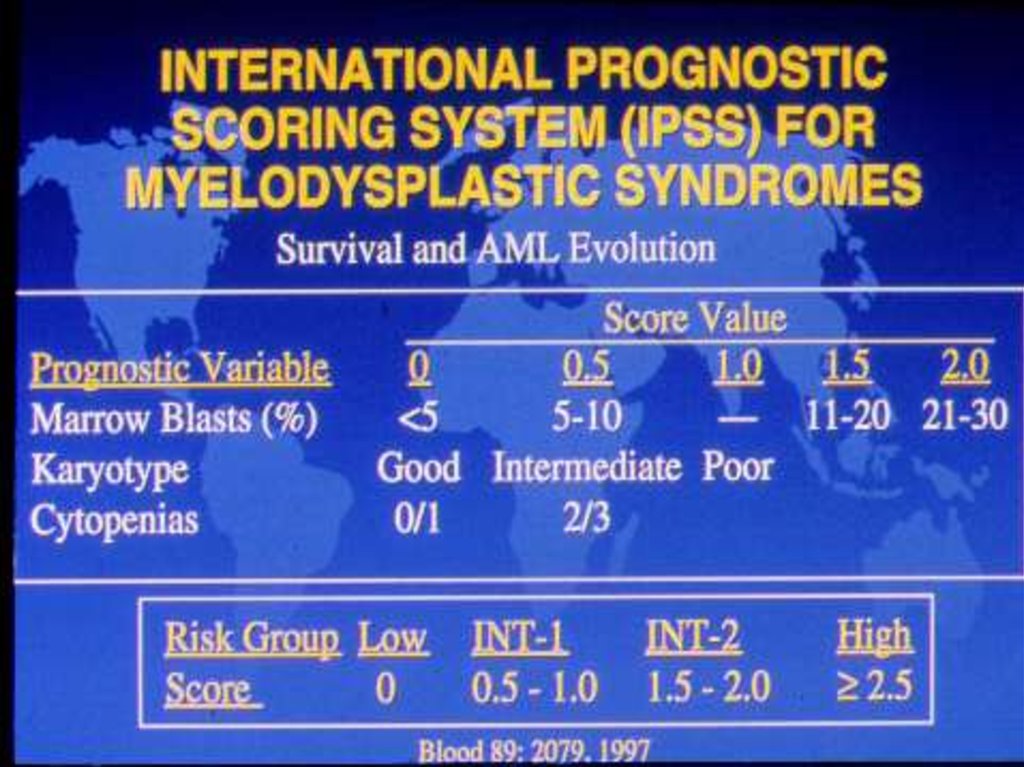
23. PROGNOSTIC INDICATORS IN MDS
• Age• Gender
• Bone marrow blast %
• # of cytopenias
• Cytogenetics
24. Cytogenetics in prognosis of MDS
GOOD normalY5q20INTERMEDIATE
Other abn.
POOR
Complex (>3
abn.)
Chr. 7 abn.
25. DIFFERENTIAL DIAGNOSIS OF MDS
• Non-neoplastic causes ofmyelodysplasia
• Neoplastic Diseases
• Megaloblastic changes
• Chronic
• Toxic agents, i.e., heavy
myeloproliferative
disease
• Acute myeloid
leukemia
metals, acute alcohol
intoxication
• Drug effects
• Congenital dyserythropoietic
anemia
• Chronic infectious disease
• Acquired immunodeficiency
syndrome (AIDS)
26. PROBLEM AREAS IN THE DISTINCTION OF MDS AND AML
• Borderline blast counts• Cases with >50% erythroid precursors
• Cases with criteria of MDS with a
cytogenetic abnormalities specific for AML
(Rosati S, Anastasi J, Vardiman J. Sem Hematol 23:
27. DISTINCTION OF MDS FROM CHRONIC MYELOPROLIFERATIVE DISORDERS
MDSCMPD
Cytopenias
Normal or elevated blood
Ineffective hematopoiesis
Dysplasia
No splenomegaly
counts
Effective hematopoiesis
No dysplasia
Splenomegaly
28. WHO CLASSIFICATION OF MYELODYSPLASTIC/ MYELOPROLIFERATIVE DISEASE
• Chronic Myelomonocytic Leukemia (CMML)• Atypical Chronic Myeloid Leukemia (aCML)
• Juvenile Myelomonocytic Leukemia (JMML)
• Myelodysplastic/Myeloprolilferative Disease,
Unclassifiable
29. CHRONIC MYELOMONOCYTIC LEUKEMIA
• Bridges MDS and MPD• Persistant monocytosis >1.0
X 109/L
• No Ph1 chromosome or
BCR/ABL
• <20% blasts
• Dysplasia or clonal
chromosome abnormality or
persistent monocytosis for >3
months old and other causes
excluded
• Splenomegaly in 30 to 50%
of cases
30. ATYPICAL CHRONIC MYELOID LEUKEMIA (aCML)
↑WBC with mature andmaturing granulocytes
Low percent of monocytes
Includes rare cases of BCRABL negative leukemia
comprised of mature and
maturing granulocytes
High leukocyte count MDS
or chronic
myeloproliferative
syndrome with
myelodysplastic features
31. JUVENILE MYELOMONOCYTIC LEUKEMIA (JMML)
• Synonymous with JCML• 60% of patients >2 year old
• Ph chromosome and BCR-ABL
negative
• Hepatosplenomegaly,
lymphadenopathy
• Skin involvement - café-au-lait
spots - NF
• Usually prominent monocytic
component
• ↑ Leukocytes, ↓ platelets
• Elevated hemoglobin F
• Usually normal cytogenetics
32. MONOSOMY 7 SYNDROME
• Anemia and leukocytosis• Thrombocytopenia in 50%
• Monocytosis
• Defective neutrophil function with
recurrent infections
• Hypercellular BM with ↑ reticulin
• Dysplasia
• Hepatosplenomegaly
• Neurofibromatosis
33. OTHER MORPHOLOGIC FINDINGS IN MDS
• Changes in marrow cellularityusually hypercellular
• Increased iron stores
• Myelofibrosis
34. MDS/MPD, UNCLASSIFIABLE
• Features of MDS but with thrombocytosis(>600 X 109/L) or leukocytosis (>13.0 X 109/L)
• (and) No prior history of MDS or MPD
• (and) No cytogenetic abnormality
associated with specific myeloid disorder
• (or) Mixed MDS and MPD features and
cannot be assigned to any other category
35. Treatment
Supportive care – blood products, infectionsetc.
Growth factors – G-CSF, erythropoetin
Hypomethylating agents – azacitidin,
dacogen
Revlimid – 5qAllogeneic stem cell transplantation
36. Myeloid Clonal Hemopathies: Evolutions
37.
38.
39.
40.
41.
42. Survival Based on WPSS Malcovati et al, ASH 05, #788
L et al. Blood. 2005;106:232a [abstract 788]43. WPSS for MDS: Clinical Outcomes Malcovati et al, ASH 12/05 #788a
Risk / ScoreSurvival
AML evolution
Very Low / 0
11.3 yr
7%@10yr
Low / 1
5.3
-
Intermediate/2
3.7
-
High / 3-4
1.6
-
Very High / 5-6
0.7
50%@8mo