








")












































")






")










")


















")


")















")
")
")
")









 Медицина
МедицинаПохожие презентации:






")



Basics of EKG Interpretation
1. Basics of EKG Interpretation
Arnold Seto, MD, MPAChief of Cardiology
Long Beach VA Medical Center
2. Outline
1.2.
3.
4.
5.
Review of the conduction system
QRS breakdown
Rate
Axis
Rhythms
3. The Normal Conduction System
4. Waveforms and Intervals
5. EKG Leads
The standard EKG has 12 leads:3 Standard Limb Leads
3 Augmented Limb Leads
6 Precordial Leads
The axis of a particular lead represents the viewpoint from
which it looks at the heart.
6. Standard Limb Leads
7. All Limb Leads
8. Precordial Leads
Adapted from: www.numed.co.uk/electrodepl.html9. Precordial Leads
10. Anatomic Groups (Summary)
11. Rate
► Rule► 10
of 300
Second Rule
12. Rule of 300
Take the number of “big boxes” betweenneighboring QRS complexes, and divide this
into 300. The result will be approximately
equal to the rate
Although fast, this method only works for
regular rhythms.
13. What is the heart rate?
www.uptodate.com(300 / 6) = 50 bpm
14. What is the heart rate?
www.uptodate.com(300 / ~ 4) = ~ 75 bpm
15. What is the heart rate?
(300 / 1.5) = 200 bpm16. The Rule of 300
It may be easiest to memorize the following table:# of big
boxes
Rate
1
300
2
150
3
100
4
75
5
60
6
50
17. 10 Second Rule
As most EKGs record 10 seconds of rhythm perpage, one can simply count the number of beats
present on the EKG and multiply by 6 to get the
number of beats per 60 seconds.
This method works well for irregular rhythms.
18. What is the heart rate?
The Alan E. Lindsay ECG Learning Center ; http://medstat.med.utah.edu/kw/ecg/33 x 6 = 198 bpm
19. The QRS Axis
By near-consensus, thenormal QRS axis is defined
as ranging from -30° to +90°.
-30° to -90° is referred to as a
left axis deviation (LAD)
+90° to +180° is referred to as
a right axis deviation (RAD)
20. Determining the Axis
► TheQuadrant Approach
► The
Equiphasic Approach
21. Determining the Axis
PredominantlyPositive
Predominantly
Negative
Equiphasic
22. The Quadrant Approach
1. Examine the QRS complex in leads I and aVF to determineif they are predominantly positive or predominantly
negative. The combination should place the axis into one
of the 4 quadrants below.
23. The Quadrant Approach
2. In the event that LAD is present, examine lead II todetermine if this deviation is pathologic. If the QRS in II is
predominantly positive, the LAD is non-pathologic (in other
words, the axis is normal). If it is predominantly negative, it
is pathologic.
24. Quadrant Approach: Example 1
The Alan E. LindsayECG Learning Center
http://medstat.med.utah.
edu/kw/ecg/
Negative in I, positive in aVF RAD
25. Quadrant Approach: Example 2
The Alan E. LindsayECG Learning Center
http://medstat.med.utah.
edu/kw/ecg/
Positive in I, negative in aVF
Predominantly positive in II
Normal Axis (non-pathologic LAD)
26. The Equiphasic Approach
1. Determine which lead contains the most equiphasic QRScomplex. The fact that the QRS complex in this lead is
equally positive and negative indicates that the net
electrical vector (i.e. overall QRS axis) is perpendicular to
the axis of this particular lead.
2. Examine the QRS complex in whichever lead lies 90° away
from the lead identified in step 1. If the QRS complex in
this second lead is predominantly positive, than the axis of
this lead is approximately the same as the net QRS axis. If
the QRS complex is predominantly negative, than the net
QRS axis lies 180° from the axis of this lead.
27. Equiphasic Approach: Example 1
The Alan E. Lindsay ECG Learning Center ; http://medstat.med.utah.edu/kw/ecg/Equiphasic in aVF Predominantly positive in I QRS axis ≈ 0°
28. Equiphasic Approach: Example 2
The Alan E. Lindsay ECG Learning Center ; http://medstat.med.utah.edu/kw/ecg/Equiphasic in II Predominantly negative in aVL QRS axis ≈ +150°
29. Systematic Approach
► Rate► Rhythm
► Axis
► Wave
Morphology
P, T, and U waves and QRS
complex
► Intervals
PR, QRS, QT
► ST Segment
30. Rhythms/Arrhythmias
► Sinus► Atrial
► Junctional
► Ventricular
31. Sinus Rhythms: Criteria/Types
►Pwaves upright in I, II, aVF
► Constant
P-P/R-R interval
► Rate
► Narrow
► P:QRS
► P-R
QRS complex
ratio 1:1
interval is normal and constant
32. Sinus Arrhythmias: Criteria/Types
► NormalSinus Rhythm
► Sinus
Bradycardia
► Sinus
Tachycardia
► Sinus
Arrhythmia
33. Normal Sinus Rhythm
• Rate is 60 to 10034. Sinus Bradycardia
• Can be normal variant• Can result from medication
• Look for underlying cause
35. Sinus Tachycardia
• May be caused by exercise, fever,hyperthyroidism
• Look for underlying cause, slow the rate
36. Sinus Arrhythmia
• Seen in young patients• Secondary to breathing
• Heart beats faster
37. Atrial Arrhythmias: Criteria/Types
►Pwaves inverted in I, II and aVF
► Abnormal
shape
Notched
Flattened
Diphasic
► Narrow
QRS complex
38. Atrial Arrhythmias: Criteria/Types
► Premature► Ectopic
Atrial Contractions
Atrial Rhythm
► Wandering
► Multifocal
Atrial Pacemaker
Atrial Tachycardia
► Atrial
Flutter
► Atrial
Fibrillation
39. Premature Atrial Contraction
• QRS complex narrow• RR interval shorter than sinus QRS
complexes
• P wave shows different morphology
than sinus P wave
40. Ectopic Atrial Rhythm
• Narrow QRS complex• P wave inverted
41. Wandering Atrial Pacemaker
• 3 different P wave morphologiespossible with ventricular rate < 100 bpm
42. Multifocal Atrial Tachycardia
• 3 different P wave morphologieswith ventricular rate> 100 bpm
43. Atrial Flutter
• Regular ventricular rate 150 bpm• Varying ratios of F waves to QRS
complexes, most common is 4:1
• Tracing shows 2:1 conduction
44. Atrial Flutter
• Tracing shows 6:1 conduction45. Atrial Fibrillation
• Tracing shows irregularly irregularrhythm with no P waves
• Ventricular rate usually > 100 bpm
46. Atrial Fibrillation
• Tracing shows irregularly irregularrhythm with no P waves
• Ventricular rate is 40
47. Atrial Tachycardia
• Tracing shows regular ventricular ratewith P waves that are different from sinus
P waves
• Ventricular rate is usually 150 to 250 bpm
48. Junctional Arrhythmias: Criteria
AV Nodal Blocks• Delay conduction of impulses from
sinus node
• If AV node does not let impulse
through, no QRS complex is seen
• AV nodal block classes:
1st, 2nd, 3rd degree
49. Junctional Arrhythmias: Criteria
1st Degree AV Block• PR interval constant
• >.2 sec
• All impulses conducted
50. Junctional Arrhythmias: Types
nd2
Degree AV Block Type 1
• AV node conducted each impulse
slower and finally no impulse is
conducted
• Longer PR interval, finally no QRS
complex
51. Premature Junctional Contractions
nd2
Degree AV Block Type 2
• Constant PR interval
• AV node intermittently conducts
no impulse
52. Junctional Escape Rhythm
rd3
Degree AV Block
• AV node conducts no impulse
• Atria and ventricles beat at intrinsic
rate (80 and 40 respectively)
• No association between P waves and
QRS complexes
53. Accelerated Junctional Tachycardia
Another Consideration:Wolfe-Parkinson-White (WPW)
• Caused by bypass
tract
• AV node is bypassed,
delay
• EKG shows short PR
interval <.11 sec
• Upsloping to QRS
complex (delta wave)
54. Junctional Tachycardia
WPW• Delta wave, short PR interval
55. AV Nodal Reentrant Tachycardia (AVNRT)
Ventricular Arrhythmias:Criteria/Types
► Wide
QRS
complex
► Rate
:
variable
► No
P waves
► Premature
Ventricular
Contractions
► Idioventricular
► Accelerated
Rhythm
IVR
► Ventricular
Tachycardia
► Ventricular
Fibrillation
56. Rate Summary
Premature Ventricular Contraction• Occurs earlier than sinus beat
• Wide, no P wave
57. AV Nodal Blocks
Idioventricular Rhythm• Escape rhythm
• Rate is 20 to 40 bpm
58. 1st Degree AV Block
Accelerated Idioventricular Rhythm• Rate is 40 to 100 bpm
59. 2nd Degree AV Block Type 1
Ventricular Tachycardia• Rate is > than 100 bpm
60. 2nd Degree AV Block Type 2
Torsades de Pointes• Occurs secondary to prolonged
QT interval
61. 3rd Degree AV Block
Ventricular Tachycardia/Fibrillation• Unorganized activity of ventricle
62. Another Consideration: Wolfe-Parkinson-White (WPW)
Ventricular Fibrillation63. WPW
Chamber Enlargements64. Ventricular Arrhythmias: Criteria/Types
Left Ventricular Hypertrophy (LVH)► Differential
Diagnosis
Hypertension (HTN)
Aortis Stenosis (AS)
Aortic Insufficiency (AI)
Hypertrophic Cardiomyopathy (HCM)
Mitral Regurgitation (MR)
Coarctation of the Aorta (COA)
Physiologic
65. Premature Ventricular Contraction
Left Ventricular Hypertrophy (LVH)► False
positive
Thin chest wall
Status post mastectomy
Race, Sex, Age
Left Bundle Branch Block (LBBB)
Acute MI
Left Anterior Fascicular Block
Incorrect standardization
66. Idioventricular Rhythm
EKG Criteria: Diagnosis of LVH67. Accelerated Idioventricular Rhythm
LVH with Strain68. Ventricular Tachycardia
Right Ventricular Hypertrophy► Reversal
of precordial pattern
R waves prominent in V1 and V2
S waves smaller in V1 and V2
S waves become prominent in V5
V6
and
69. Torsades de Pointes
Right Ventricular Hypertrophy70. Ventricular Tachycardia/Fibrillation
Right Ventricular Hypertrophy:Causes
► Chronic
Obstructive Pulmonary Disease
► Pulmonary HTN
Primary
► Pulmonary Embolus
► Mitral Stenosis
► Mitral Regurgitation
► Chronic LV failure
71. Ventricular Fibrillation
Right Ventricular Hypertrophy:Causes
► Tricuspid
► Atrial
Regurgitation
Septal Defect
► Pulmonary
► Tetralogy
Stenosis
of Fallot
► Ventricular
Septal Defect
72. Chamber Enlargements
Left Atrial Enlargement: Causes► Mitral
Stenosis
► Mitral
Regurgitation
► Left
ventricular hypertrophy
► Hypertension
► Aortic
Stenosis
► Aortic
Insufficiency
► Hypertrophic
Cardiomyopathy
73. Left Ventricular Hypertrophy (LVH)
Left Atrial Enlargement: Criteria►P
wave
► Notch
in P wave
Any lead
Peaks > 0.04 secs
► V1
Terminal portion of P wave > 1mm deep
and > 0.04 sec wide
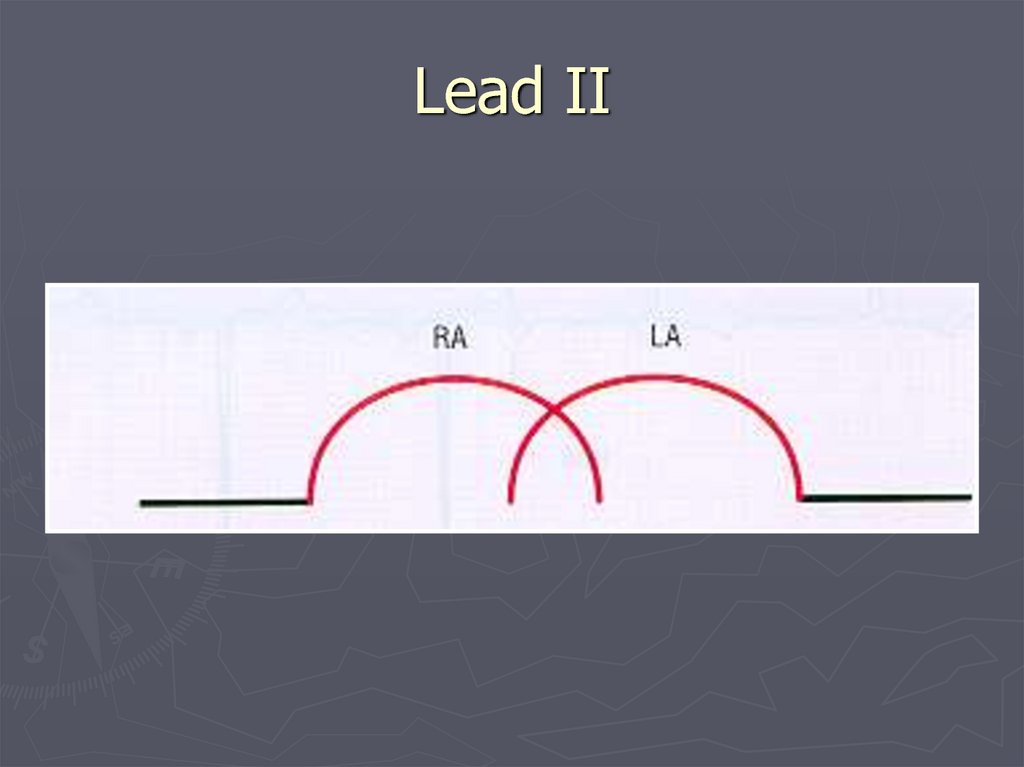
74.
Lead II75. EKG Criteria: Diagnosis of LVH
P Wave: Left Atrial Enlargement76. EKG Criteria
Left Atrial EnlargementLead V1
77. LVH with Strain
Right Atrial Enlargement: Causes► CHD
Tricuspid Stenosis
Pulmonary Stenosis
► COPD
► Pulmonary
HTN
► Pulmonary
Embolus
► Mitral
Regurgitation
► Mitral
Stenosis
78. Right Ventricular Hypertrophy
Right Atrial Enlargement: Criteria► Tall,
peaked P wave
> 2.5 mm in any lead
► Most
prominent P waves in leads I, II
and aVF
79. Right Ventricular Hypertrophy
Right Atrial Enlargement80. Right Ventricular Hypertrophy: Causes
Bundle Branch Blocks81. Right Ventricular Hypertrophy: Causes
Bundle Branch Blocks► Left
Complete
Incomplete
► Right
Complete
Incomplete
► Complete
QRS > .12 secs
► Incomplete
QRS .10 - .12 secs
82. Left Atrial Enlargement: Causes
Left Bundle Branch Block: Causes► Normal
variant
► Idiopathic
degeneration of the
conduction system
► Cardiomyopathy
► Ischemic
► Aortic
heart disease
Stenosis
► Hyperkalemia
► Left
Ventricular Hypertrophy
83. Left Atrial Enlargement: Criteria
Criteria for Left Bundle BranchBlock (LBBB)
► Bizarre
QRS Morphology
High voltage S wave in V1, V2 & V3
Tall R wave in leads I, aVL and V5-6
► Often LAD
► QRS Interval
► ST depression in leads I, aVL, & V5-V6
► T wave inversion in I, aVL, & V5-V6
84. Lead II
Left Bundle Branch Block85. P Wave: Left Atrial Enlargement
Right Bundle Branch Block:Causes
► Idiopathic
degeneration of the
conduction system
► Ischemic heart disease
► Cardiomyopathy
► Massive Pulmonary Embolus
► Ventricular Hypertrophy
► Normal Variant
86. Left Atrial Enlargement Lead V1
Criteria for Right BundleBranch Block (RBBB)
► QRS
morphology
Wide S wave in leads I and V4-V6
RSR’ pattern in leads V1, V2 and V3
► QRS duration
► ST depression in leads V1 and V2
► T wave inversion in leads V1 and V2
87. Right Atrial Enlargement: Causes
Right Bundle Branch Block88. Right Atrial Enlargement: Criteria
Right Bundle Branch Block89. Right Atrial Enlargement
Anterior Septal with RBBB90. Bundle Branch Blocks
Ischemia and Infarction91. Bundle Branch Blocks
Normal Complexes and Segments92. Left Bundle Branch Block: Causes
J Point93. Criteria for Left Bundle Branch Block (LBBB)
Ischemia•T wave inversion, ST segment depression
•Acute injury: ST segment elevation
•Dead tissue: Q wave
94. Left Bundle Branch Block
Measurements95. Right Bundle Branch Block: Causes
ST-Segment Elevation96. Criteria for Right Bundle Branch Block (RBBB)
ST Segment DepressionCan be characterised as:► Downsloping
► Upsloping
► Horizontal
97. Right Bundle Branch Block
EKG Changes: Ischemia →Acute Injury→ Infarction
98. Right Bundle Branch Block
Evolution of TransmuralInfarction
99. Anterior Septal with RBBB
100. Ischemia and Infarction
Evolution of a SubendocardialInfarction
101. Normal Complexes and Segments
102. J Point
Hyperacute T waves103. Ischemia
Q WavesNon Pathological Q waves
Q waves of less than 2mm are normal
Pathological Q waves
Q waves of more than 2mm
indicate full thickness myocardial
damage from an infarct
Late sign of MI (evolved)
104. Measurements
Look for Grouped Patterns(Footprints)
► ST
Depressions = Ischemia
► ST
Elevations = injury
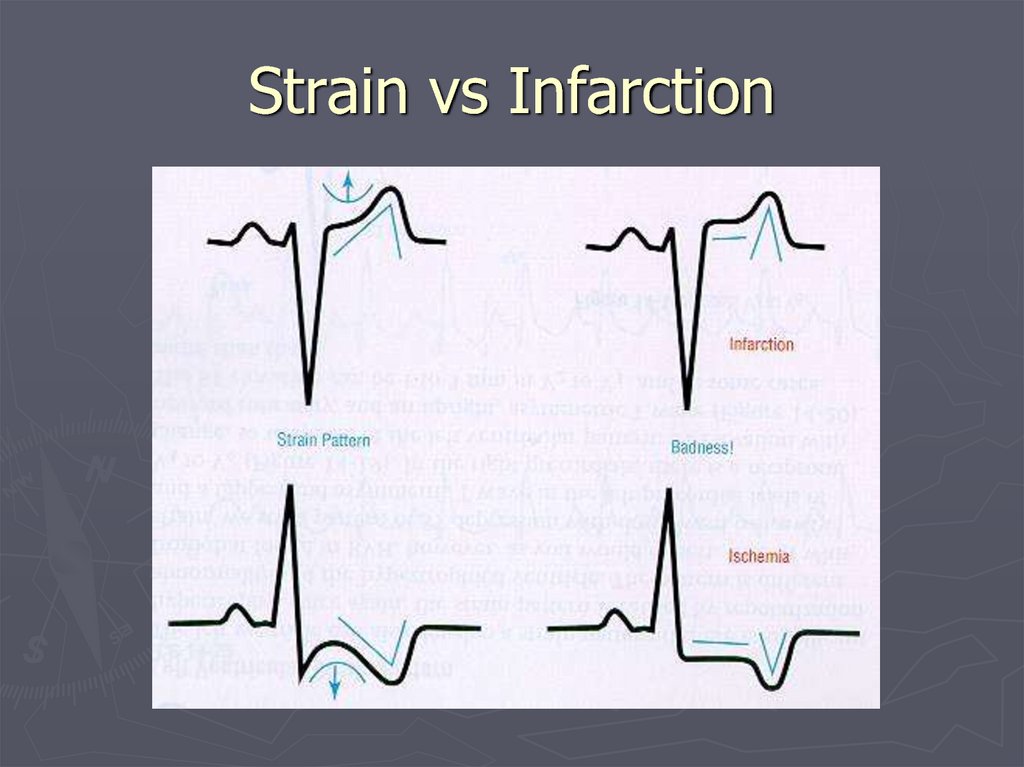
►Q
Waves & T Wave Inversion = Infarction
105. ST-Segment Elevation
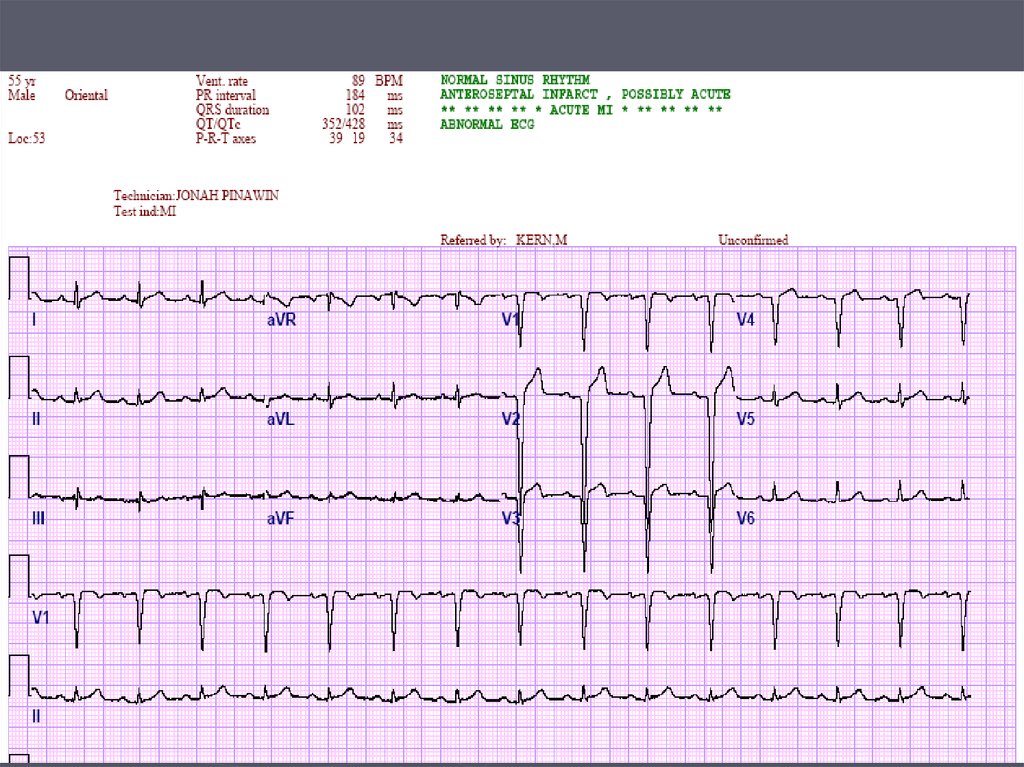
Anterior Septal (Left AnteriorDescending)
106. ST Segment Depression
Anterior Lateral (Left Circumflex)107. EKG Changes: Ischemia → Acute Injury→ Infarction
Inferior (Right Coronary Artery)108. Evolution of Transmural Infarction
109.
110. Evolution of a Subendocardial Infarction
111.
112. Hyperacute T waves
113. Q Waves
114. Look for Grouped Patterns (Footprints)
ST-T Wave Changes115. Anterior Septal (Left Anterior Descending)
Strain in Hypertrophy116. Anterior Lateral (Left Circumflex)
Strain in LVH117. Inferior (Right Coronary Artery)
Strain in RVH118.
Strain vs Infarction119.
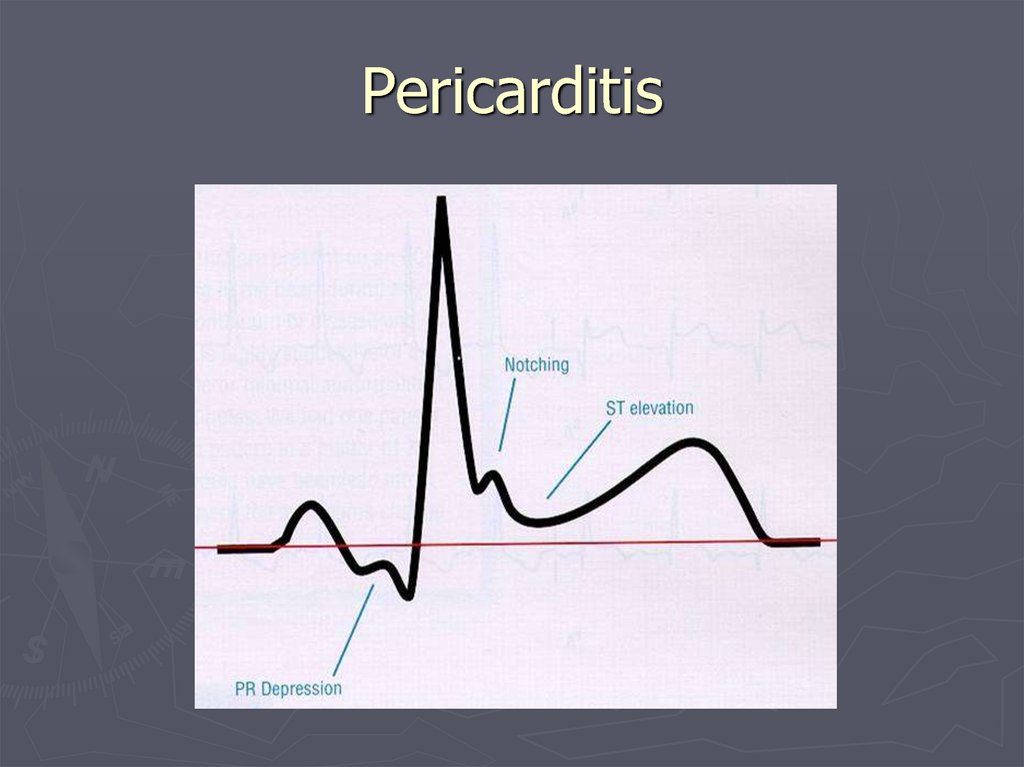
Pericarditis120.
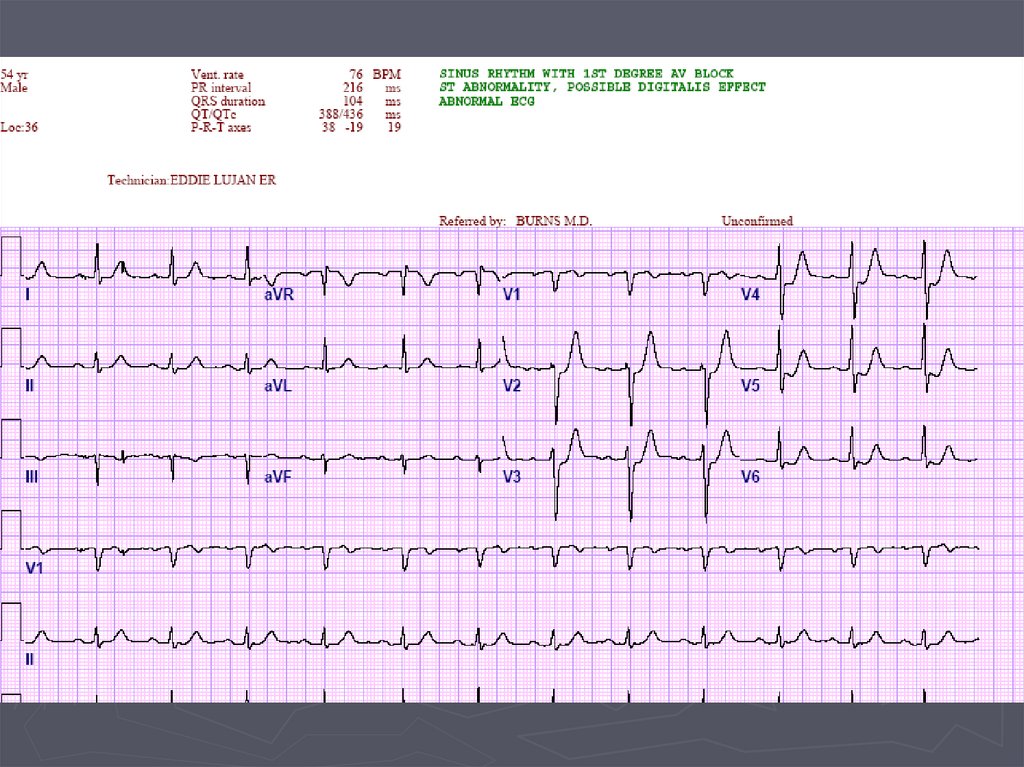
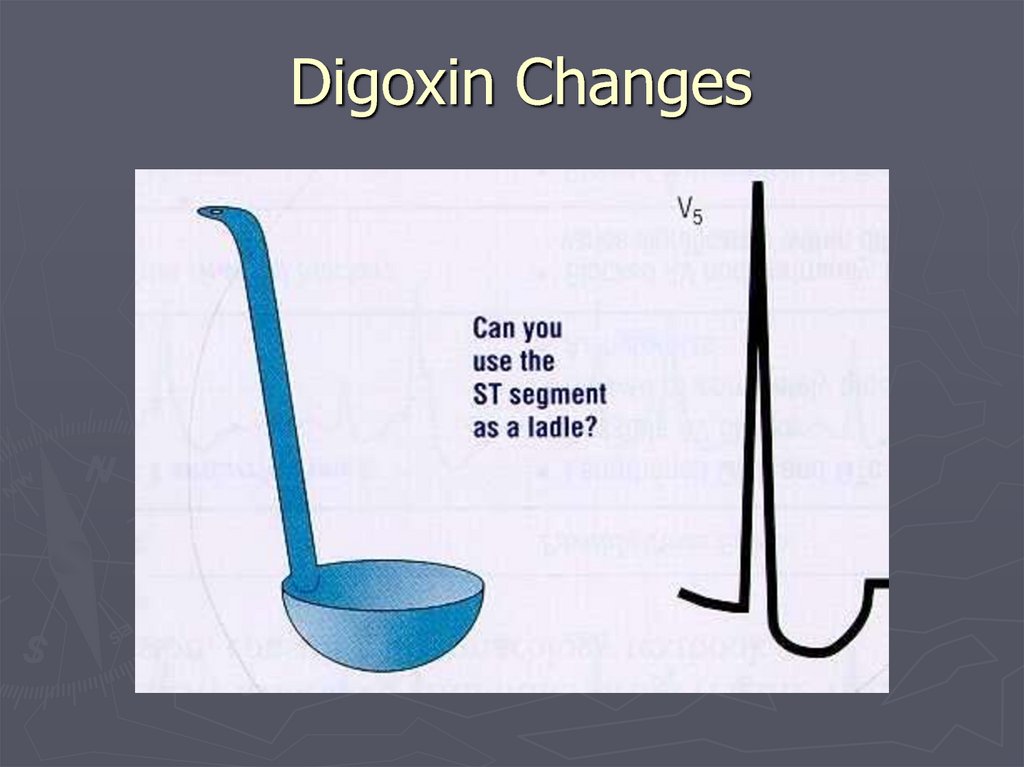
Digoxin Changes121.
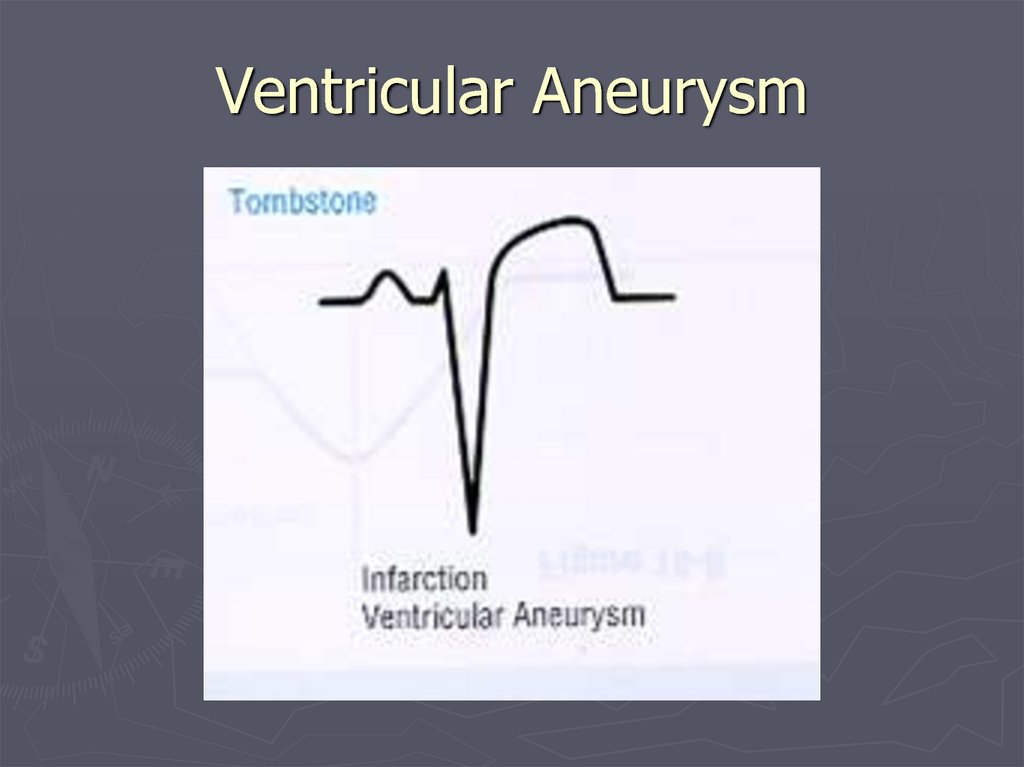
Ventricular Aneurysm122.
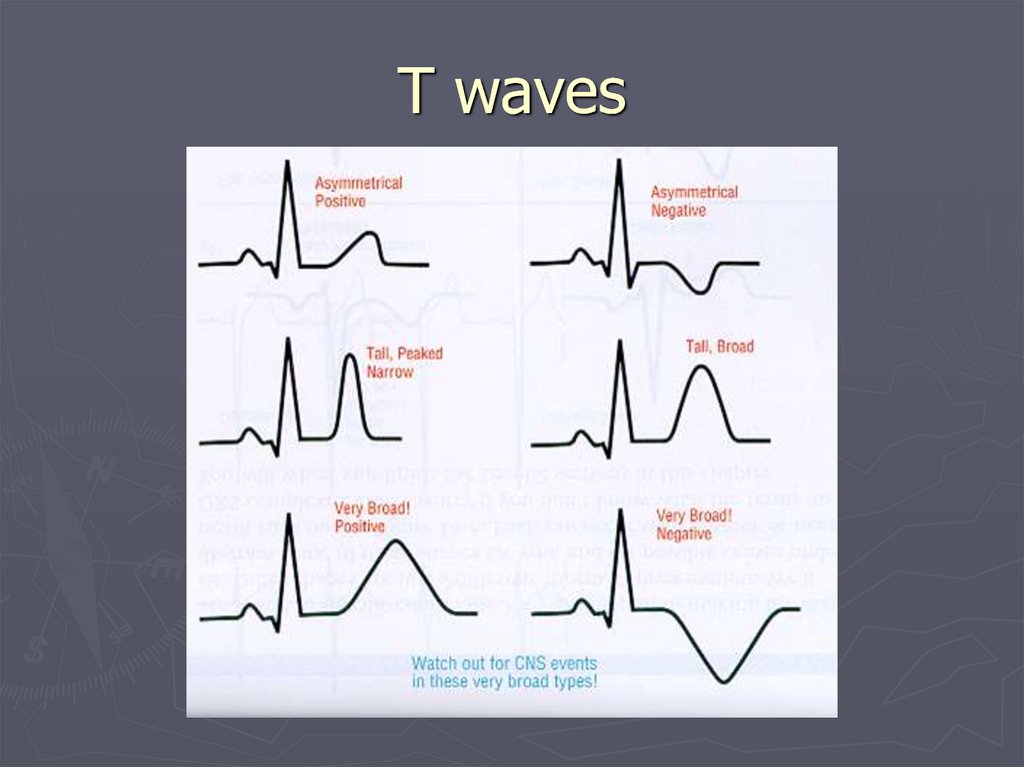
T waves123.
Summary► Basic
physiology of the conduction
system
► Origin
of a normal EKG
► Systematic
► Major
EKG
approach to reading an EKG
abnormalities when reading an