












 Медицина
МедицинаПохожие презентации:



")






Pleural Effusions and Pneumothorax
1.
Pleural Effusions andPneumothorax
2.
Pleural Effusions introduction• The movement of fluid across
the pleural membranes is
complicated but in general is
governed by Starling's law of
capillary exchange
• 5 to 10 L of fluid transgress the
pleural space over a 24-hour
period
• Under physiologic conditions,
most pleural fluid reabsorption
is through lymphatics of the
parietal pleura
3.
Pleural Effusions introduction• imbalance of accumulation and absorption of
pleural fluid will lead to the development of a
pleural effusion:
1. Increased hydrostatic pressure
2. Increased negative intrapleural pressure
3. Increased capillary permeability
4. Decreased plasma oncotic pressure
5. Decreased or interrupted lymphatic
drainage
4.
Pleural Effusions introduction• About 300 mL of fluid is required for the
development of costophrenic angle blunting
seen on an upright chest radiograph.
• At least 500 mL of effusion is necessary for
detection on clinical examination.
5.
Transudative Vs. Exudative Effusions• Criteria:
1. Pleural fluid protein/serum protein greater than 0.5
2. Pleural fluid LDH/serum LDH greater than 0.6
3. Pleural fluid LDH 1.67 times normal serum
These criteria misidentify ~25% of transudates as exudates
• A transudative pleural effusion occurs when systemic factors that
influence the formation and absorption of pleural fluid are altered.
• An exudative pleural effusion occurs when local factors that
influence the formation and absorption of pleural fluid are altered
6.
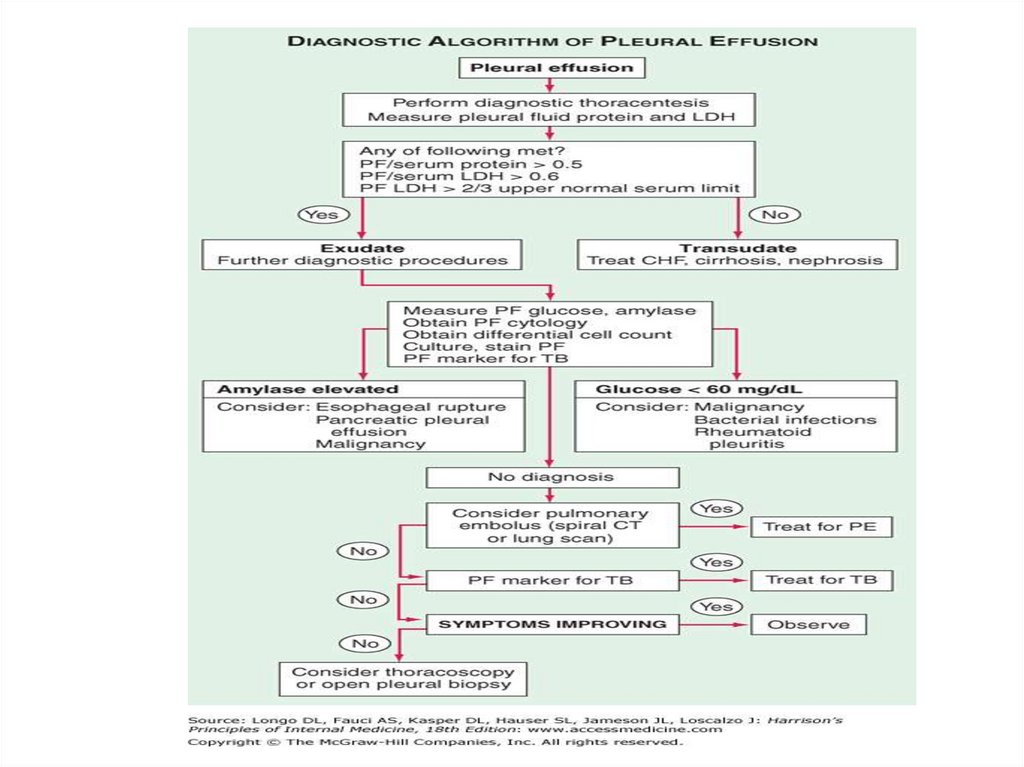
Diagnostic Approach• The leading causes of transudative pleural
effusions in the United States are leftventricular failure and cirrhosis
• The leading causes of exudative pleural
effusions are bacterial pneumonia,
malignancy, viral infection, and pulmonary
embolism.
7.
Pleural fluid analysis• Gross appearance (pus- Empyema, black- Aspergillus, greenBiliothorax, white- Chylothorax)
• Very high LDH- empyema, rheumatoid pleurisy, malignancy
• High triglyceride- Chylothorax
• Low glucose- Rheumatoid pleurisy, parapneumonic effusion or
empyema, Malignant effusion, Tuberculous pleurisy, Lupus pleuritis,
Esophageal rupture
• Low pH- parapneumonic effusion or empyema, Malignant effusion
• High amylase- Acute pancreatitis, Chronic pancreatic pleural
effusion, Esophageal rupture, Malignancy
• adenosine deaminase (ADA), interferon gamma - Tuberculous
pleurisy
• Lymphocytosis- tuberculous pleurisy, lymphoma, sarcoidosis,
chronic rheumatoid pleurisy
8.
9.
Effusion Due to Heart Failure• A diagnostic thoracentesis should be
performed if the effusions are not bilateral
and comparable in size, if the patient is febrile,
if the patient has pleuritic chest pain or if the
effusion persists despite therapy
• A pleural fluid N-terminal pro-brain natriuretic
peptide (NT-proBNP) >1500 pg/mL is virtually
diagnostic of an effusion secondary to
congestive heart failure
10.
Hepatic Hydrothorax• Pleural effusions occur in ~5% of patients with
cirrhosis and ascites
• effusion is usually right-sided
11.
Parapneumonic Effusion• Parapneumonic
effusions are
associated with
bacterial pneumonia,
lung abscess, or
bronchiectasis and
are probably the
most common cause
of exudative pleural
effusion
• Empyema refers to a
grossly purulent
effusion
12.
Parapneumonic Effusion• Patients with aerobic bacterial pneumonia and
pleural effusion present with an acute febrile
illness consisting of chest pain, sputum
production, and leukocytosis
• Patients with anaerobic infections present
with a subacute illness
• If the free fluid separates the lung from the
chest wall by >10 mm, a therapeutic
thoracentesis should be performed
13.
Uncomplicated Vs. Complicatedparapneumonic effusion
• An uncomplicated parapneumonic effusion
has "exudative" chemistries, normal pH and
glucose, and negative cultures
• A complicated parapneumonic effusion
typically has "exudative" chemistries, a low
pleural pH (pH <7.20), a low glucose, and is
often loculated
14.
Indication for pleural drainage• Loculated pleural fluid
• Pleural fluid pH <7.20
• Pleural fluid
glucose <3.3 mmol/L
(<60 mg/dL)
• Positive Gram stain or
culture of the pleural
fluid
• Presence of gross pus
in the pleural space
15.
Before and after driange16.
Treatment of parapneumonic effusion• An empiric, broad spectrum antibiotic that
includes coverage for anaerobic organisms
• In patients with an uncomplicated
parapneumonic effusion that is small to
moderate in size, free flowing, and has a pH of
7.20 or greater there is no indication for drainage
• In patients with a large, loculated, or complicated
parapneumonic effusion there is indication for
prompt drainage of any remaining pleural fluid by
chest tube.
17.
Effusion Secondary to Malignancy• Malignant pleural effusions
secondary to metastatic
disease are the second most
common type of exudative
pleural effusion
• The three tumors that cause
~75% of all malignant pleural
effusions are lung carcinoma,
breast carcinoma, and
lymphoma
18.
Effusion Secondary to Malignancy• The diagnosis usually is made via cytology of
the pleural fluid
• If the initial cytologic examination is negative,
thoracoscopy is the best next procedure if
malignancy is strongly suspected
19.
Treatment of Malignant pleuraleffusion
• If the patient's lifestyle is compromised by
dyspnea and if the dyspnea is relieved with a
therapeutic thoracentesis, one of the
following procedures should be considered:
1. therapeutic thoracentesis
2. insertion of a small indwelling catheter
3. pleurodesis
20.
Pneumothorax introduction• Pneumothorax is the accumulation of air within the pleural
space
• Pneumothorax can be spontaneous or occur secondary to a
traumatic, surgical, therapeutic, or disease-related event
• pneumothorax compresses lung tissue and reduces
pulmonary compliance, ventilatory volumes, and diffusing
capacity
• If air enters the pleural space repeatedly and is unable to
escape, positive pressure will develop in the pleural space.
This situation is called a tension pneumothorax
21.
Pneumothorax introduction• Patients with pneumothorax most commonly
present with chest pain (sharp and pleuritic)
and dyspnea
• Characteristic physical findings include:
1. Hyperresonance on percussion
2. Breath sounds are diminished to absent.
3. Subcutaneous emphysema may be palpated
22.
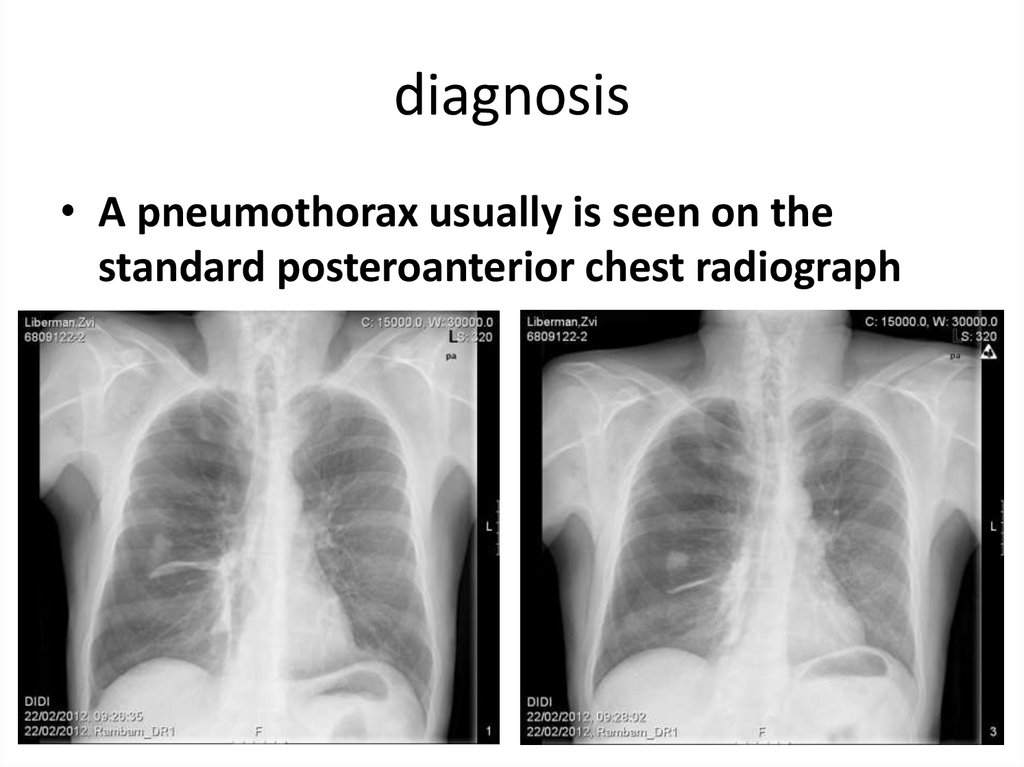
diagnosis• A pneumothorax usually is seen on the
standard posteroanterior chest radiograph
23.
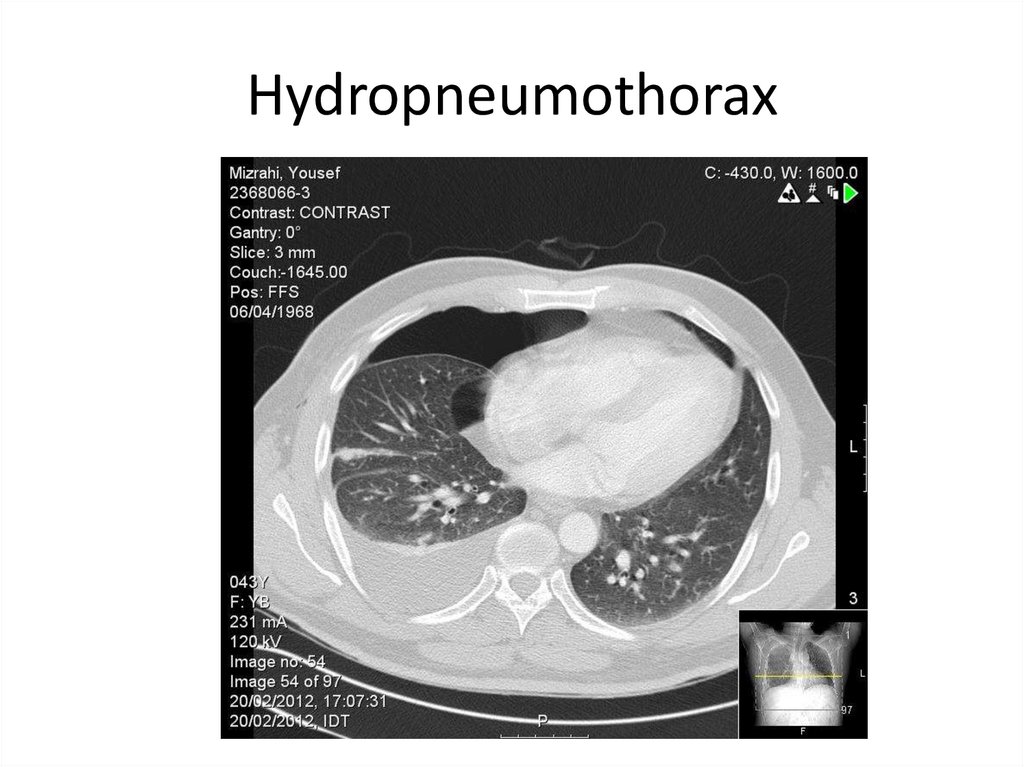
Hydropneumothorax24.
Classifications of Pneumothorax• Spontaneous
1. Primary
2. Secondary
• Traumatic
• Iatrogenic
• Esophageal perforation
25.
primary spontaneouspneumothorax
• A primary spontaneous pneumothorax occurs in the absence
of underlying lung disease
• Patients are often tall, thin and smoker men from 25 to 40
years of age (rare after age 40)
• Risk factor include: smoking, family history, Marfan
syndrome, homocystinuria, and thoracic endometriosis
• Primary spontaneous pneumothoraxes are usually due to
rupture of apical pleural blebs (>85%)
• 25-50% of patients with a first time spontaneous
pneumothorax will have a recurrence (most recurrences
occurring within the first year )
26.
Treatment of primaryspontaneous pneumothorax
• Small pneumothoraces (<20%, ≤2 to 3 cm
between the lung and chest wall on a chest
radiograph) that are stable may be monitored
if the patient has few symptoms. An
uncomplicated pneumothorax reabsorbs at a
rate of about 1% per day.
• Indications for intervention include
progressive pneumothorax, delayed
pulmonary expansion, or development of
symptoms.
27.
Treatment of primaryspontaneous pneumothorax
• Moderate (20%-40%) and large (>40%) pneumothoraces
nearly always are associated with persistent symptoms that
cause physical limitations and require intervention
• Simple needle aspiration of a pneumothorax may relieve
symptoms and can promote quicker lung re-expansion
• Tube thoracostomy (chest tube insertion) and underwater
seal drainage are the mainstays of treatment for
spontaneous pneumothorax.
• The classic location for chest tube insertion is through the
fourth, fifth, or sixth intercostal space in the mid to anterior
axillary line.
28.
Treatment of primaryspontaneous pneumothorax
• Complications of chest tube insertion for
pneumothorax are infrequent but include
laceration of an intercostal vessel, laceration
of the lung, intrapulmonary or extrathoracic
placement of the chest tube, and infection.
• When an air leak persist for more than 72
hours or the lung not completely re-expand,
surgical intervention is warranted
29.
Indication for Surgical interventionin spontaneous pneumothorax
• Air leak that persist for more than 72 hours or when
the lung not completely re-expand
• Bilateral simultaneous pneumothoraces
• Complete (100%) pneumothorax
• Pneumothorax associated with tension or
borderline cardiopulmonary reserve
• Pneumothorax in patients in high-risk professions
or activities
• A recurrence pneumothorax
30.
Surgical intervention forspontaneous pneumothorax
• Apical blebs are resected. The parietal pleura
over the apex of the hemithorax can be
removed (pleurectomy), abraded (mechanical
pleurodesis), or treated with talc or
tetracycline-like agents (chemical pleurodesis
or poudrage).
• The recurrence rate of these procedures,
performed open or closed, is less than 5%
31.
Secondary spontaneouspneumothorax
• Most secondary pneumothoraxes are due to
chronic obstructive pulmonary disease
• Pneumothorax in patients with lung disease is
more life-threatening than it is in normal
individuals because of the lack of pulmonary
reserve in these patients.
• Treatment of secondary pneumothorax is very
similar to PSP but most of the patients with
secondary pneumothorax should be treated
with tube thoracostomy.
32.
Preventing recurrence• smoking cessation
• VATS pleurodesis- The rate of recurrent
pneumothorax is less than 5 percent after
VATS with bleb/bullae resection and
pleurodesis
• Chemical pleurodesis- decreases the
recurrence rate for pneumothorax to 15-25%
33.
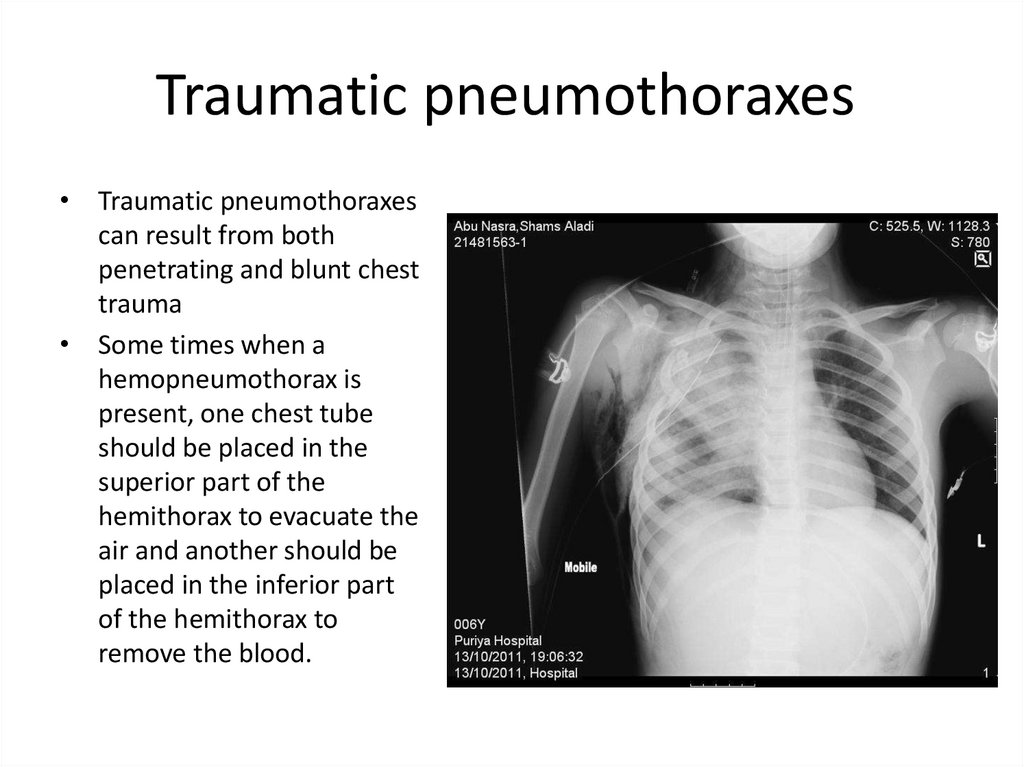
Traumatic pneumothoraxes• Traumatic pneumothoraxes
can result from both
penetrating and blunt chest
trauma
• Some times when a
hemopneumothorax is
present, one chest tube
should be placed in the
superior part of the
hemithorax to evacuate the
air and another should be
placed in the inferior part
of the hemithorax to
remove the blood.
34.
Traumatic pneumothoraxes35.
Iatrogenic pneumothoraxIatrogenic pneumothorax is a type of traumatic pneumothorax that is
becoming more common. The leading causes are transthoracic needle
aspiration, thoracentesis, and the insertion of central intravenous
catheters.
36.
tension pneumothorax• hemodynamic collapse (decreased venous
return to the heart and reduced cardiac
output)
• severe respiratory compromise
• compression or collapse of the entire lung
• shifting of the mediastinum and heart away
from the pneumothorax
37.
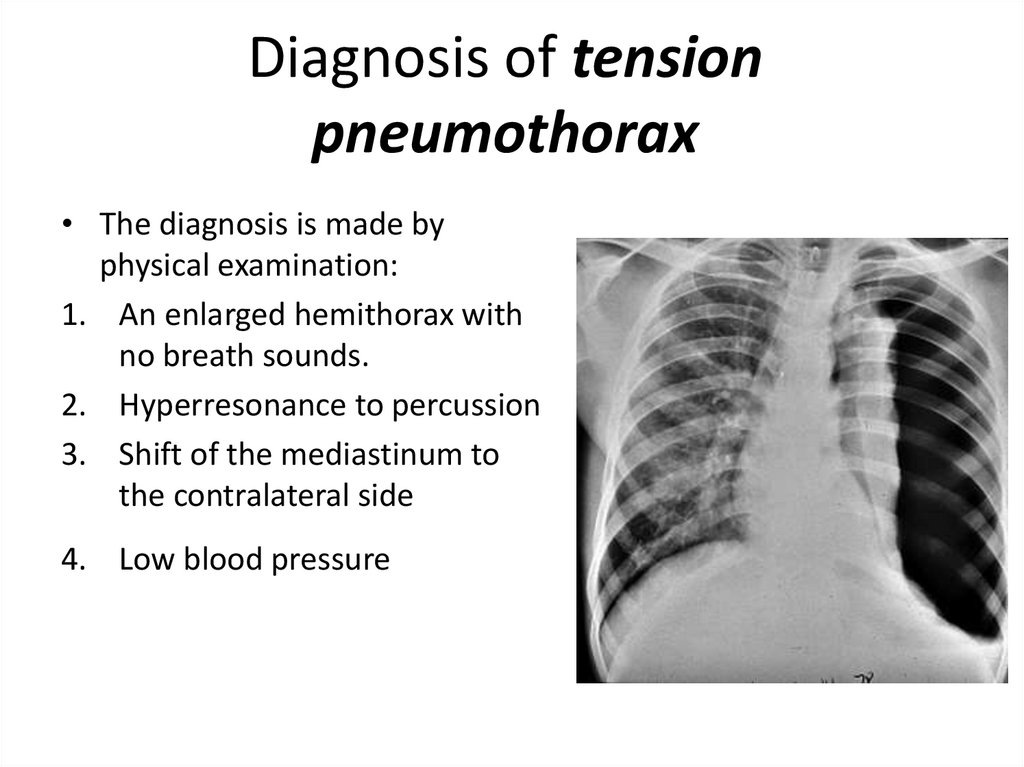
Diagnosis of tensionpneumothorax
• The diagnosis is made by
physical examination:
1. An enlarged hemithorax with
no breath sounds.
2. Hyperresonance to percussion
3. Shift of the mediastinum to
the contralateral side
4. Low blood pressure
38.
Treatment of tensionpneumothorax
• Tension pneumothorax must be treated as a
medical emergency
• A large-bore needle should be inserted into
the pleural space through the second anterior
intercostal space.
• The needle should be left in place until a
thoracostomy tube can be inserted