










 Медицина
МедицинаПохожие презентации:










Basics in organization of family medicine in Ukraine and Worldwide
1. “Basics in organization of family medicine in Ukraine and Worldwide”
ZSMUDepartment of general practice – family
medicine
“Basics in organization of
family medicine in Ukraine
and Worldwide”
2.
First term primary health care (PHC) is foundin scientific studies of Lord Dowson (1920, UK),
Millis, Willard (1960-1969, USA), and M.
Lflonde (1974, Canada), which mentioned in
their writings about PHC, but none of them gave
a definition of this concept.
In May 1978 at the International Conference on
PHC, held in Alma-Ata, the World Health
Organization (WHO) first defines the concept of
PHC, which indicated the priority PHC and
affected the national system of health care
around the world.
3.
1. New Londonfamily medical
center
2. Charlestown
center of a
family medicine
4.
3. Family medicine center Hamptons. USA5.
6.
Family medicine in the world continues todevelop.
Today, the development of a family
medicine in the world has achieved
considerable success, especially in
Europe.
Switching health care systems in many
European countries on the principles of a
family medicine has proved its efficiency
and economic benefits.
7.
Were created powerfulinternational association of family
doctors WONCA and regional
(European, Asian, South American,
North American, and others).
They periodically hold international
conferences and congresses where new
achievements and successes of family
medicine in the world are illuminated.
8.
World Organization of National Colleges, Academies - Wonca• World Organization of Family Doctors (WONCA)
founded in 1972;
• consists of national colleges, academies and
organizations of general practitioners / family doctors.
• Now it counts about 300,000 members representing
126 organizations from 102 countries.
WONCA President
Prof Richard G Roberts
WONCA Еurope President
Anthony Mathie
9.
The main aim of Wonca is theimprovement of living standards by:
• raising service standards in family
medicine,
• promoting intensive exchange of
information,
• support scientific and clinical research,
and
• the development of educational
standards.
10.
WorkgroupsEducation (EURACT)
Research
Environment
Ethical Issues
Informatics
Women and Family Medicine
Mental Health
High-quality and safe care
Rural Practice
WICC (International
Classification)
Special Interest Groups
Cancer and Palliative Care
Difficulties in Health
Geriatric help
Medicine of migration and
tourism
international health
International Movement of family
doctors Vasco da Gama
includes 32 countries
Purpose:
Holding conferences and
exchange programs for young
family doctors
Identifying problems of young
family doctors and finding their
solutions
Participation in the development
of measures to improve the
quality of education
cooperation with all WONCA
Institutions.
11.
• General practice / family medicine is anacademic and scientific discipline with its
own purpose, objectives, research methods,
evidence base and clinical activity.
Family Medicine is a separate discipline
rather than a set of parts of other disciplines
because it requires its own scientific base.
• Research is an integral part of any scientific
discipline (they are also part of family
medicine).
(European Wonca, 2002, 2005)
12.
13.
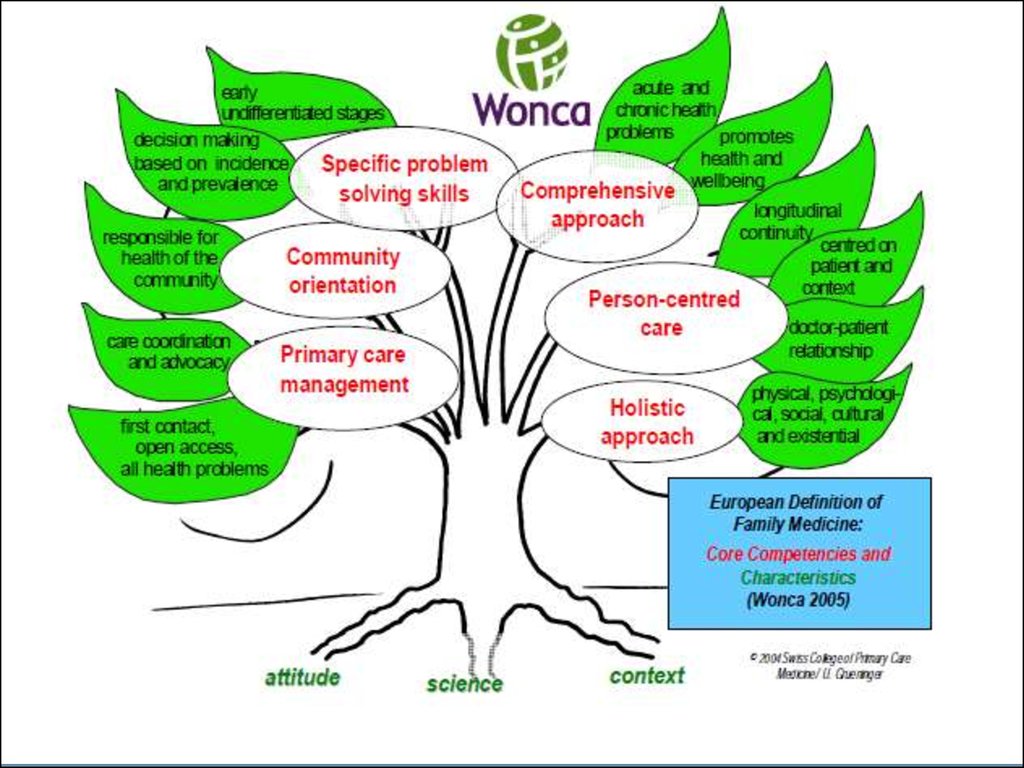
Competence of a GP – Family doctor1. Management of primary care :
- first contact,
- open and unrestricted access,
-help with all the health problems
-effective use of resources through the coordination of
assistance and cooperation with other primary care
professionals,
-managing the interface between general and specific
help,
-take the role of defender of the patient when needed, ie ,
to protect patients from harm that may be inflicted as a
result of unnecessary investigation and treatment
(European Wonca, 2005)
14.
Competence of a GP – Family doctor2. Patient-centered care:
- focused on the individual, his / her family,
- establishing a long relationship,
- effective communication,
-long continuous assistance
3. Addressing specific problems :
-making specific decisions,
-the prevalence of certain accident must cope
simultaneously considering individual approach with
both acute and chronic health problems with at all
stages,
-a wide range of complaints and illnesses, comorbidities
(European Wonca, 2005)
15.
4. A comprehensive approach:- control disease stage differentiation diagnosis,
- risk management and probabilities,
- health promotion and prevention as important as
cure,
- care and palliative care
5. Targeting Society: responsible for public health
6. Holistic approach:
health problems in their biomedical, psychological,
social, culture and
existential dimension
16.
Characteristics of general practice - familymedicine:
1. Available for the entire population primary
care, most often - on the line of first contact
with the patient's health care system, which
solved the problem of the patient, regardless of
age, sex and other characteristics;
2. Ensures efficient use of resources of the entire
health system by coordinating the efforts of
various specialists, as well as by patients' rights
when necessary;
17.
Characteristics of general practice - familymedicine:
3. Provides individual assistance to the patient,
but with the characteristics of his family and
social environment;
4. Has a unique opportunity consulting all
family members, regardless of age, examines the
state of health of the family in several generations.
Based on effective relationship between doctor
and family.
18.
5. Responsible for the consistency and continuityof care, according to the patient's needs;
6. Has its own unique type of clinical thinking
and decision-making path, which is determined by
statistical and epidemiological indicators of health
and illness;
7. Solves the problem of diseases in preclinical
often non-differentiable stage;
19.
8. Solves both the problem of acute and chronicdiseases;
9. Personalized counseling on maintaining a
healthy lifestyle;
10. Responsible for the quality and effectiveness
of care provided to the individual as well as to the
community;
11. Solve health problems in their physical,
psychological, social, cultural and existential
definitions;
20.
Diagnostic techniques include- interviewing the patient to collect
information on the present symptoms,
- prior medical history and other health details,
followed by a physical examination.
Many FDs are trained in basic medical testing:
interpreting results of blood or other patient
samples,
electrocardiograms, or x-rays
More complex and time-intensive diagnostic
procedures are usually obtained by referral
to specialists, due to either special training
with a technology, or increased experience and
patient volume that renders a risky procedure
safer for the patient.
21.
After collecting data, the FD:- arrives at a differential diagnosis and, with
the participation of the patient,
-formulates a plan including components of
further testing,
- specialist referral,
- medication, therapy, diet or life-style
changes
- patient education, and follow up results of
treatment.
FD also counsel and educate patients on
safe health behaviors, self-care skills and
treatment options, and provide screening
tests and immunizations
22.
Educational program and program of research ingeneral practice / family medicine
23.
Models of the family doctorpractice in the world
1. Private Practice: physician and nurses.
2. Group practice when several doctors
grouped, saving money, organize
interchangeably among themselves, to some
specialization of medical practice.
3. Medical centers (Scandinavian model),
which is actually a clinic of a GP,
sometimes a hospital for the elder patients.
24.
USA MEDICINE• The share of GP is nearly 40%
• Every year on health care 14% of the
gross national product consumed, or
almost 3 thousand dollars per 1 inhabitant.
• Average salary of a family doctor is from
44 to 60 thousand dollars a year.
• At 49.7 - 60-hour weeks (47.4 weeks per
year) FD takes about 175-182 patients and
makes 27 visits to hospital.
25.
MEDICINE in CANADA• The relationship between family doctors
and narrow specialists is 50:50.
• 3 of 4 Canadians surveyed prefer to get
any medical help from a family doctor in
the first place.
• In a small town with a population of about
4,000 people there are surgeon, internist
and 6 competent GP.
• They work as well in a local hospital with
capacity of 60-80 beds.
26.
MEDICINE in CANADA• FD spend their morning in the hospital after
12 pm works with patients in his office,
which has laboratory equipment (from
elementary to advanced studies), daily intake
25-40 patients who prefer to visit doctor in
his office.
• When hospitalization is necessary, FD assists
with helping a patient during the whole
period of staying in the hospital.
• Usually FD has 60 or more hours a week,
visiting 182 patients.
27.
MEDICINE in United Kingdom
The share of FD is about 70%
Every citizen registered in the list of specific FD
Each FD usually gives more than 8 000 consultations
per year
Approximately 85% of the consultations held in the
office of the FD, 5% and 10% home visit, and by
phone
The patient usually can not be consulted by a doctor
of secondary level (eg, hospital), without referring to a
FD in a first place.
About 13% of the population each year seek treatment
in inpatient institutions, 50% of which require
emergency measures.
28.
France medicine• This system is ranked as №1 in the WHO
rating
• FD number is 65 000
• Any medical care, except emergency,
performed only after the patient’s visit to FD
• It’s only possible to buy medicines prescribed
by a FD
• Only students with the highest level of
success can become narrow specialists,
others are FD
29.
The main problems of familymedicine
• To create algorithms, based on
scientific data obtained at the
primary stages
• To develop research protocols
• To conduct research projects that
reflect the nature and problems of
discipline.