










 Медицина
МедицинаПохожие презентации:










Heart auscultation
1.
Heart auscultationFOR 3-D YEAR STUDENTS
2.
SoundsHeart sounds occur as a result of vibration of
heart structures and blood with a sharp
slowdown or acceleration of intracardiac blood
flow
Heart sounds represent a short sound
3.
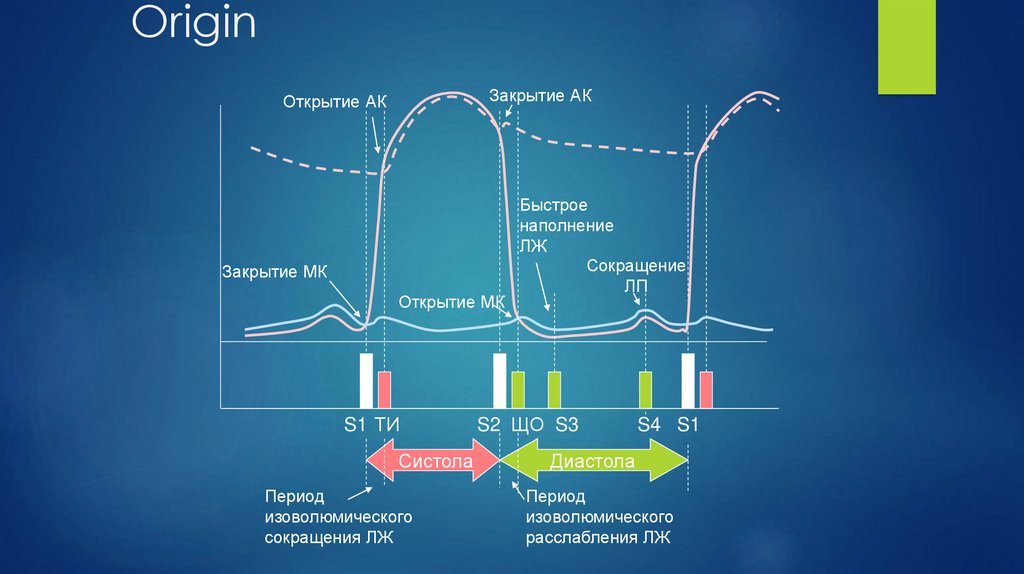
OriginЗакрытие АК
Открытие АК
Закрытие МК
Открытие МК
S1 ТИ
Систола
Период
изоволюмического
сокращения ЛЖ
Быстрое
наполнение
ЛЖ
Сокращение
ЛП
S2 ЩО S3
S4 S1
Диастола
Период
изоволюмического
расслабления ЛЖ
4.
5.
Ist heart soundit depends on:
1.
The position of the leaflets before closing
2.
Ventricular rate and force
3.
Leaflets mobility
6.
II heart soundIt depends on:
1.
Leaflets mobility
2.
Blood pressure in aorta or pulmonary artery
3.
Valve condition
7.
Normal heart sounds ratioI
II
I II
2 - 2-d i/c space right (АV)
I II
I II
3 - 2-d i/c space left (PA)
5 – 3-4 i/c space (АV)
I
II
I II
4 - xiphoid process (ТV)
I
II
1 - apex (MV)
I
II
8.
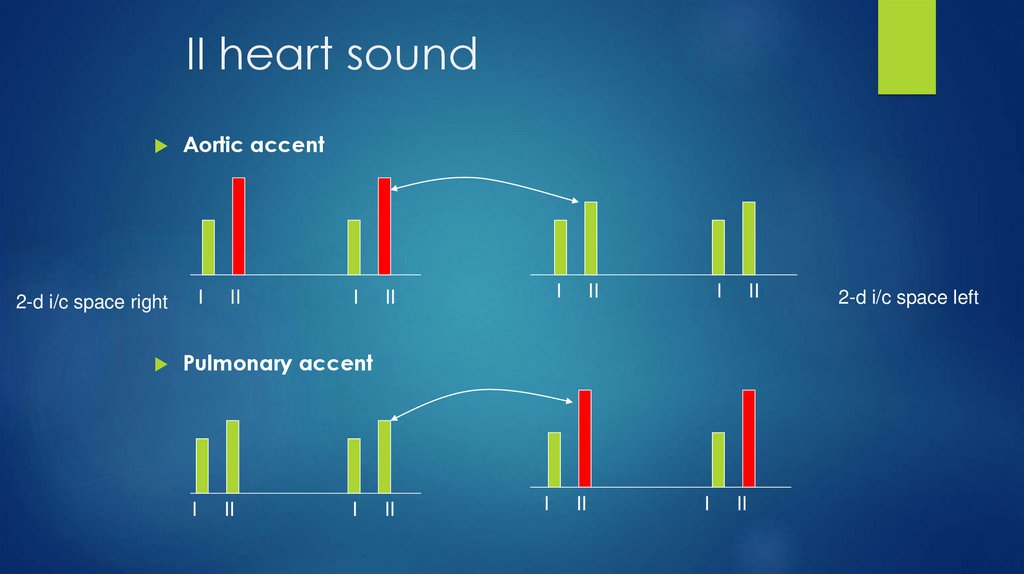
II heart soundAortic accent
I
2-d i/c space right
II
I
I
II
II
I
II
Pulmonary accent
I
II
I
II
I
II
I
II
2-d i/c space left
9.
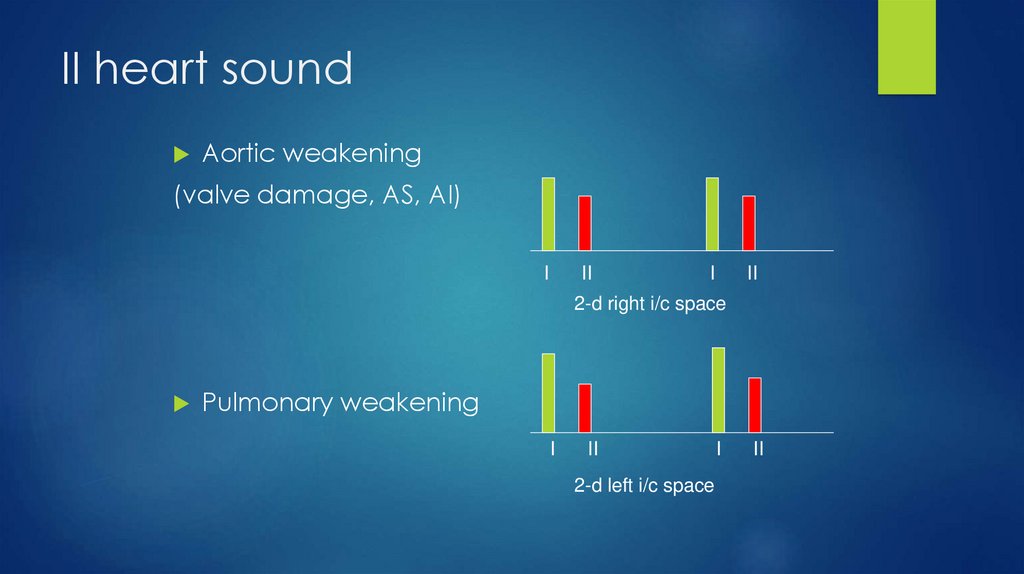
II heart soundAortic weakening
(valve damage, АS, АI)
I
II
I
II
2-d right i/c space
Pulmonary weakening
I
II
2-d left i/c space
I
II
10.
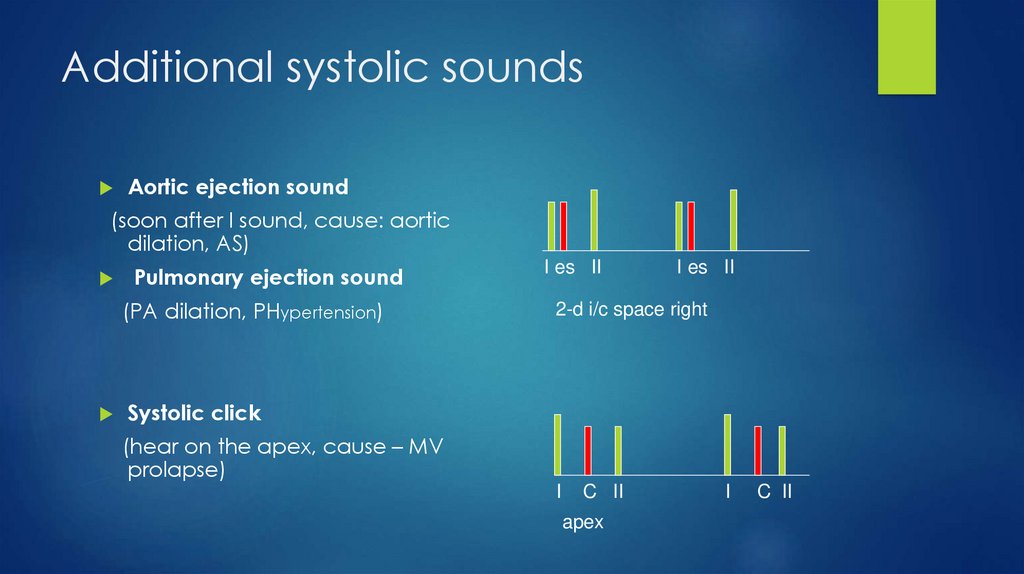
Additional systolic soundsAortic ejection sound
(soon after I sound, cause: aortic
dilation, AS)
Pulmonary ejection sound
(PA dilation, PHypertension)
I es II
I es II
2-d i/c space right
Systolic click
(hear on the apex, cause – MV
prolapse)
I
C II
apex
I
C II
11.
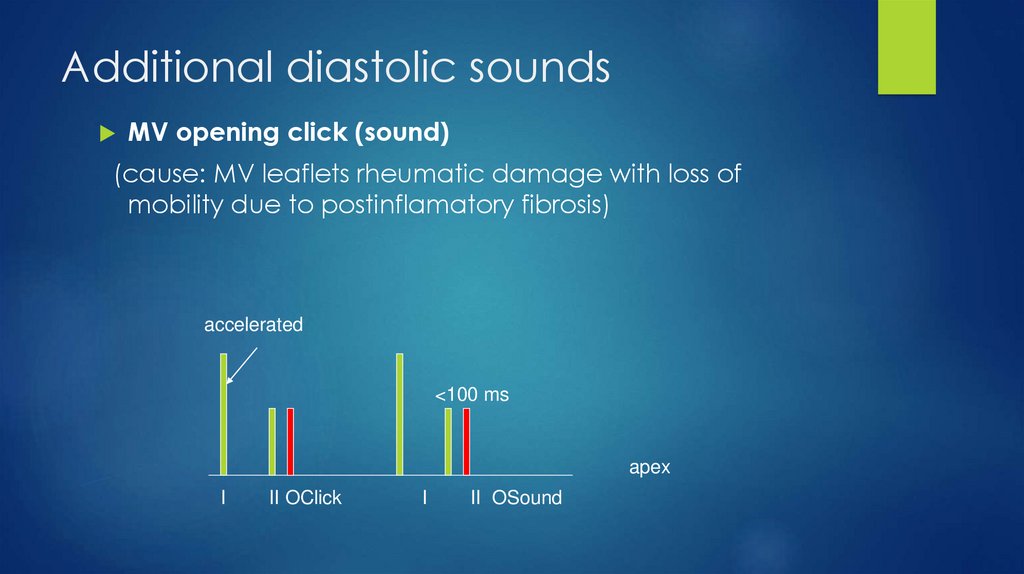
Additional diastolic soundsMV opening click (sound)
(cause: MV leaflets rheumatic damage with loss of
mobility due to postinflamatory fibrosis)
accelerated
<100 ms
apex
I
II OClick
I
II OSound
12.
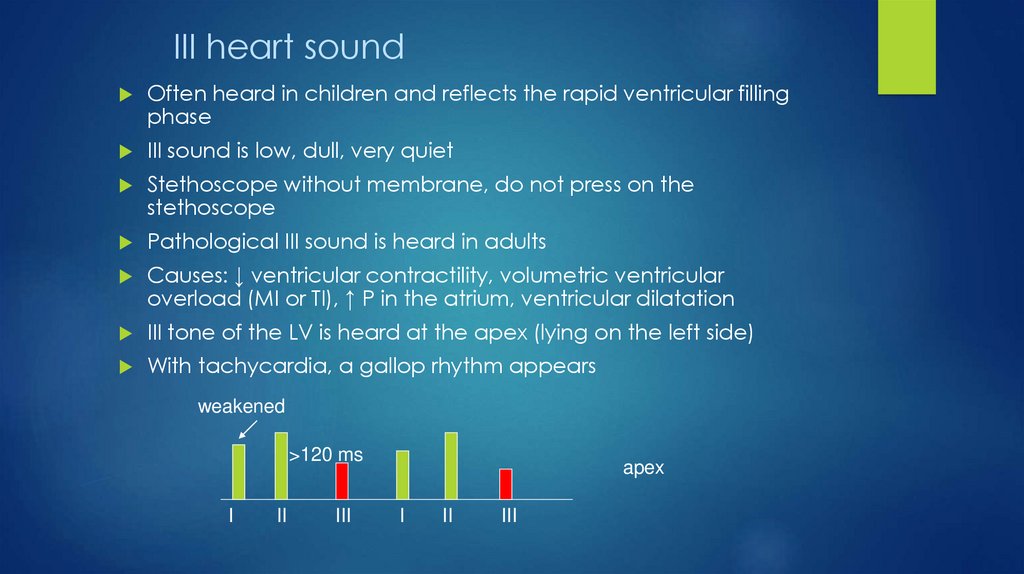
III heart soundOften heard in children and reflects the rapid ventricular filling
phase
III sound is low, dull, very quiet
Stethoscope without membrane, do not press on the
stethoscope
Pathological III sound is heard in adults
Causes: ↓ ventricular contractility, volumetric ventricular
overload (MI or TI), ↑ P in the atrium, ventricular dilatation
III tone of the LV is heard at the apex (lying on the left side)
With tachycardia, a gallop rhythm appears
weakened
>120 ms
I
II
III
apex
I
II
III
13.
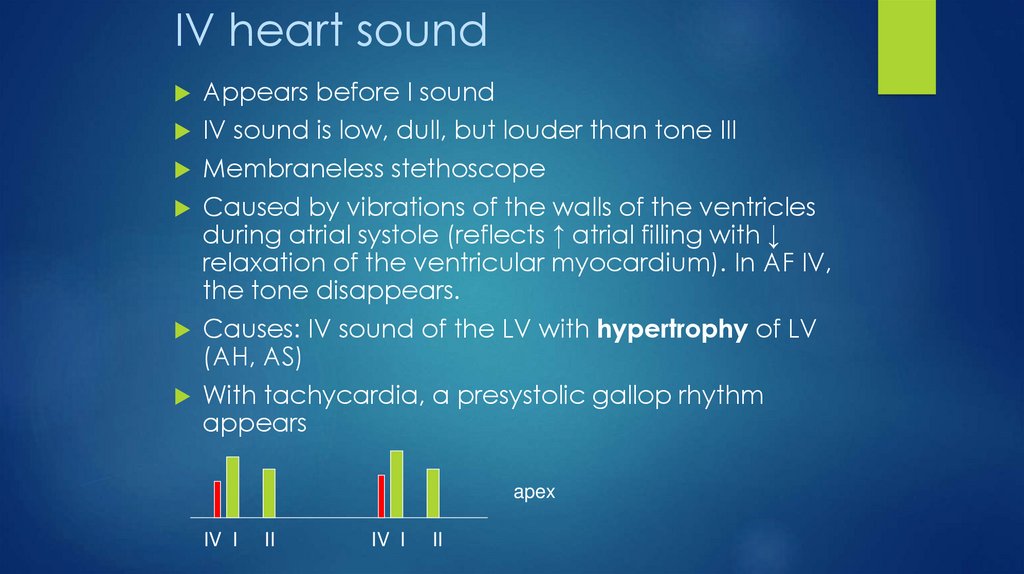
IV heart soundAppears before I sound
IV sound is low, dull, but louder than tone III
Membraneless stethoscope
Caused by vibrations of the walls of the ventricles
during atrial systole (reflects ↑ atrial filling with ↓
relaxation of the ventricular myocardium). In AF IV,
the tone disappears.
Causes: IV sound of the LV with hypertrophy of LV
(AH, AS)
With tachycardia, a presystolic gallop rhythm
appears
apex
IV I
II
IV I
II
14.
Heart noises / murmursMurmurs are caused by turbulent blood flow
and vibration
Murmurs appear and disappear when the
pressure gradient arises between the
chambers of the heart or between the
chambers and large vessels.
15.
Origin1.
Blood flow through the constricted area (AS,
MS)
2.
Acceleration of blood flow through normal
structures (↑ SV with anemia, thyreotoxicosis)
3.
Blood flow to the enlarged area (aortic
aneurysm)
4.
Regurgitation with valve failure
16.
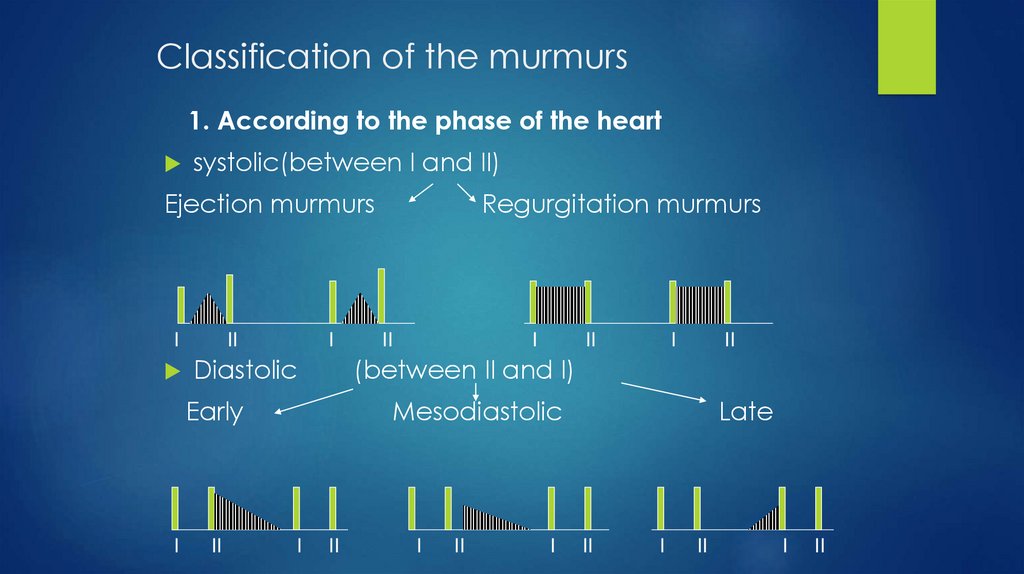
Classification of the murmurs1. According to the phase of the heart
systolic(between I and II)
Ejection murmurs
I
II
I
Diastolic
II
II
I
II
I
II
(between II and I)
Early
I
Regurgitation murmurs
Mesodiastolic
I
II
I
II
I
Late
II
I
II
I
II
17.
2. Shape - determined by the change in noise intensityRising (crescendo)
Decreasing (diminuendo)
Diamond-shaped
Plateau
3. Localization - zone of maximum noise intensity
4. Irradiation
5. Loudness (6-point score)
1 - very weak
2 - quiet
3 - moderately loud
4 - loud (jitter appears)
5 - very loud (not tight attachment of the stethoscope)
6 - very loud (no stethoscope attached)
6. Frequency (height)
7. Character
18.
Mesosystolic murmursMid-systole murmurs (ejection murmurs) are the most
common type of murmur
Peak in the middle of systole and disappear before tone II
Heard on the base of the heart (2 i/c space)
May be functional
19.
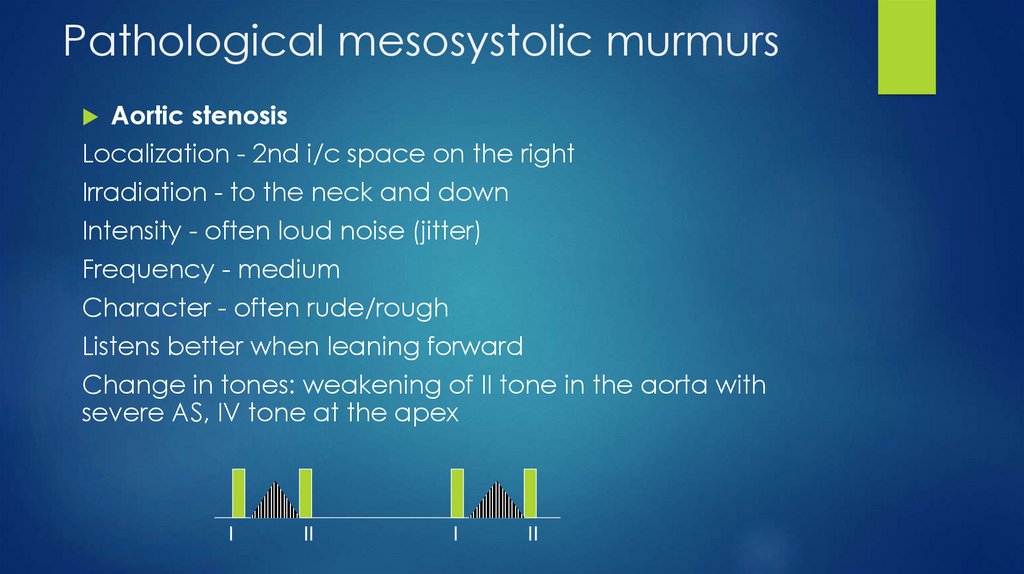
Pathological mesosystolic murmursAortic stenosis
Localization - 2nd i/c space on the right
Irradiation - to the neck and down
Intensity - often loud noise (jitter)
Frequency - medium
Character - often rude/rough
Listens better when leaning forward
Change in tones: weakening of II tone in the aorta with
severe AS, IV tone at the apex
I
II
I
II
20.
Pansystiolic murmursPansystolic murmurs pathological
Appear when blood flows from a high-pressure chamber
to a low-pressure chamber through an opening valves
that must be closed
The noise appears simultaneously with the I tone and
continues until the appearance of the II tone
21.
Mitral insufficiencyLocalization: apex
Irradiation: in left axillary region
Intensity: different
I
II
I
Height: medium or high
Character: blowing
Changes in tones: I tone is often muted, III tone
Tricuspid Insufficiency
Localization: low part of left sternum border
Intensity: different
Height: medium
Character: blowing
Inspiration lead to increase of noise intensity
Sound changes: RV III tone
II
22.
Diastolic murmursDiastolic murmurs are always pathological
Early DM of diminuendo appear due to
regurgitation with semilunar valve insufficiency
Medium and late DM appear with AV valve
stenosis
23.
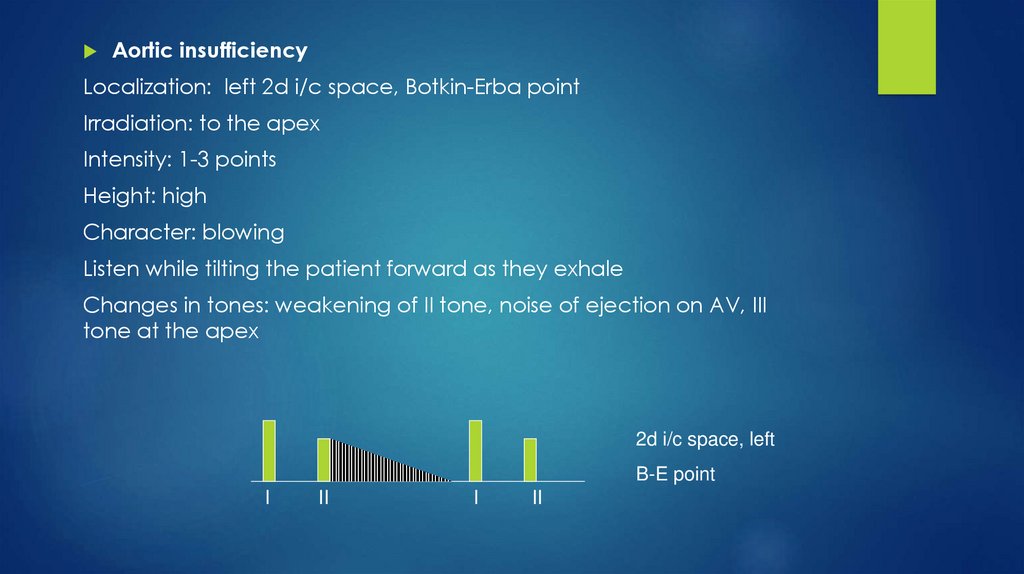
Aortic insufficiencyLocalization: left 2d i/c space, Botkin-Erba point
Irradiation: to the apex
Intensity: 1-3 points
Height: high
Character: blowing
Listen while tilting the patient forward as they exhale
Changes in tones: weakening of II tone, noise of ejection on AV, III
tone at the apex
2d i/c space, left
B-E point
I
II
I
II
24.
Mitral stenosisLocalization: apex
Irradiation: no
Intensity: 1-4
Height: low (stethoscope without membrane!)
Character: rude
Listen on left sideways, during exhalation
Tone changes: I tone clapping (accelerated),
opening click, accent of II tone on LA
I
II OC
I
II OC
25.
Functional murmursFunctional murmurs are heard in the
absence of heart pathology, usually occur
when blood is expelled through the
semilunar valves (usually PAV)
FM is mainly ejection murmurs (mesosystolic)
with a normal II tone, heard on the base, do
not radiate, quiet (1-3 points)
FM is heard in 70% of children and 50% of
adults
26.
Heart auscultation, rulesClear definition of I and II tones
Revealing additional tones
Listening to systolic murmurs
Listening to diastolic murmurs
Listening with a stethoscope with a membrane (I and II
tones, noise with AI, MI) and without a membrane (III, IV
tones, noise of MS)
Listening in phases of deep inspiration and expiration
Listening to the patient in different positions (lying, lying on
the left side (III and IV tones, mitral murmurs), sitting with an
inclination forward on exhalation (aortic murmurs),
standing)