

























 Q:")







































 Медицина
МедицинаПохожие презентации:










Valvular heart disease. Mitral valve
1.
VALVULAR HEART DISEASEMitral valve
Timur Lesbekov. MD
Chief cardiac surgery department #1
Director ECMO program
Natonal Research Cardiac Surgery Center, Astana
lesbekovt@mail.ru
heartcenter.kz
23 August 2018
2. Pathophysiological triad
3.
4. Primary valve pathology
5. Secondary valve pathology
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16. “A picture is worth a thousand words” Napoleon
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30. ECHO should give answer for 9 (at least) Q:
31.
32.
33.
34.
35. Domelike anterior leaflet movement, restriction of posterior leaflet subvalvular fusions
36.
37. Natural History of Mitral Regurgitation
Natural History ofMitral Regurgitatoo
With acute mitral regurgitation, left atrial
compliance is predominantly fixed; therefore
the left atrial pressure and pulmonary capillary
wedge pressure can rise dramatically if the
regurgitant volume is sufficiently large,
resulting in pulmonary edema.
38. Chronic Mitral Regurgitation
Chrooic Mitral RegurgitatooPatients with chronic mitral regurgitation will have a long latent period
before becoming symptomatic
39. Mitral Regurgitation hemodynamics
Mitral Regurgitatoo hemodyoamicsIn patients with significant mitral regurgitation, prominent v-waves are seen on the
left atrial pressure tracing due to simultaneous antegrade and retrograde filling of the
left atrium from pulmonary venous inflow and mitral regurgitation. With pure mitral
regurgitation, a rapid y-descent may also be present due rapid antegrade flow across
the mitral valve as a result of the elevated left atrial to left ventricular pressure
gradient
40. Symptoms
Fatgue & weakness – due to CO – predominant complaint
Exertonal dyspnea & cough – pulmonary congeston
• Palpitatons – due to atrial fbrillaton (occur in 75% of pts.)
• Edema, ascites – Right-sided heart failure
41. Sings
SiogsAtrial fbrillaton
Cardiomegally
Apical pansystolic murmur +/- thrill
Sof S1, apical S3
Signs of pulmonary venous congeston (crepitatons,
pulmonary edema, efusions)
Signs of pulmonary hypertension & right heart failure
42.
2017escardio.org
43.
Rick A. Nishimura et al. Circulaton. 2014;129:2440-249244.
45.
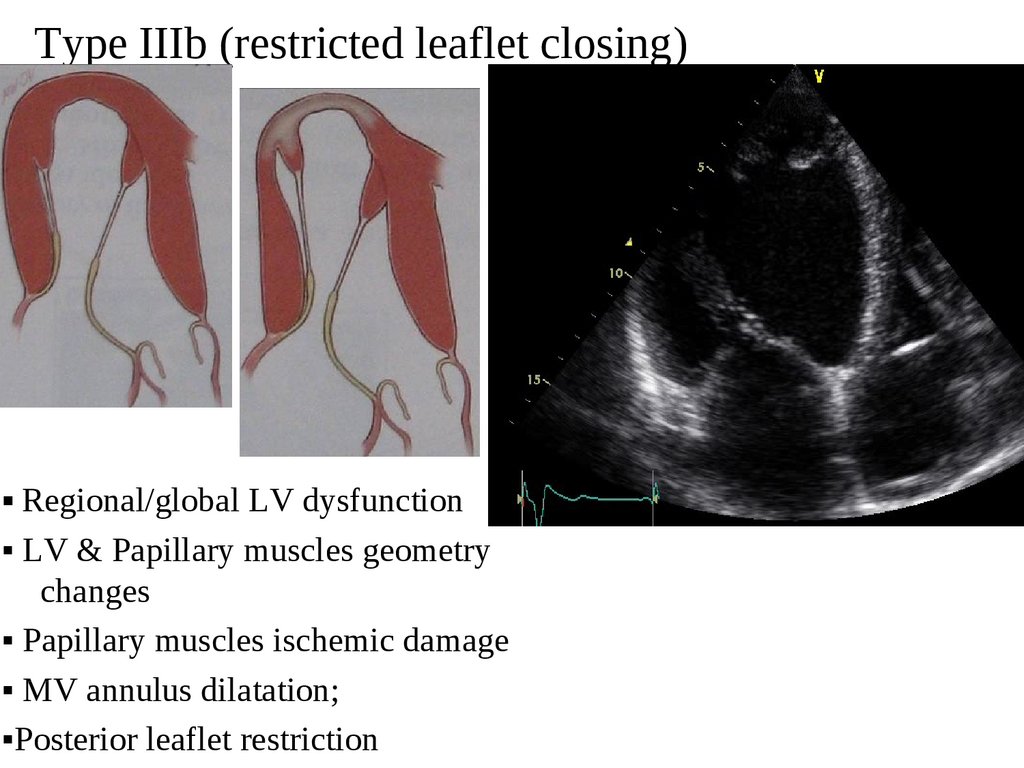
Type IIIb (restricted leaflet closing)▪ Regional/global LV dysfunction
▪ LV & Papillary muscles geometry
changes
▪ Papillary muscles ischemic damage
▪ MV annulus dilatation;
▪Posterior leaflet restriction
46.
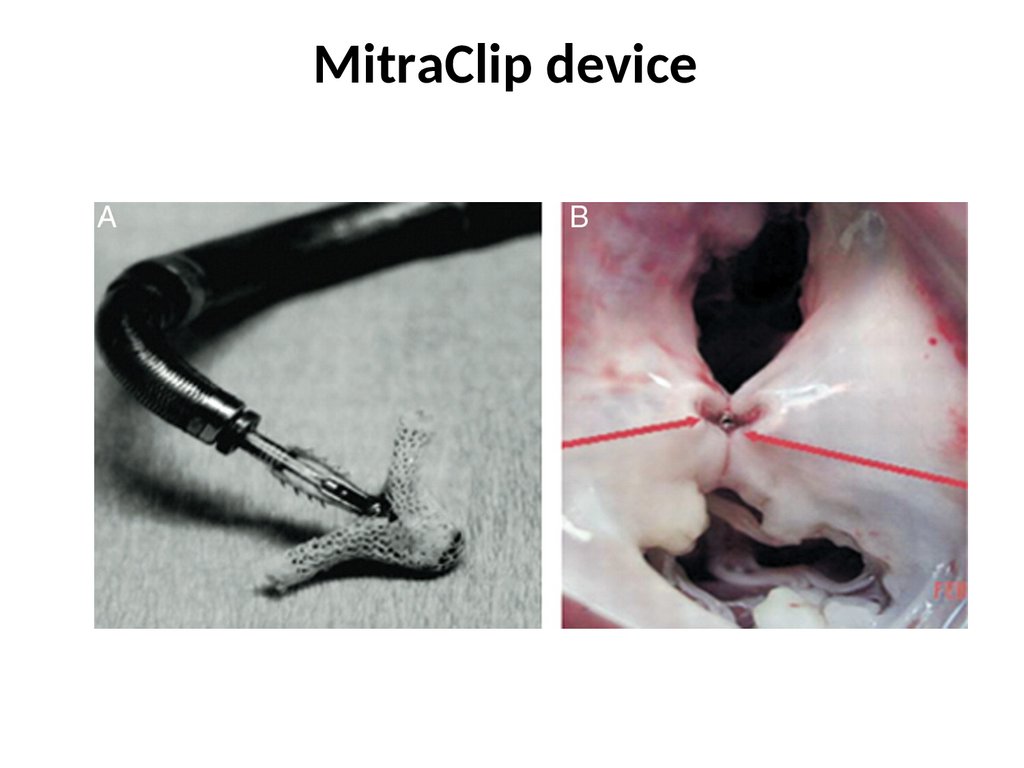
MitraClip device47.
48.
49. Mitral Stenosis
Mitral Steoosis50. Mitral Stenosis Etiologies:
Mitral Steoosis Etologies:1. Rheumatic valvular disease - the most common cause of mitral
stenosis.
2. Congenital deformities - infancy or early childhood.
2. Systemic Diseases - systemic lupus erythematosus, rheumatoid
arthritis or carcinoid syndrome.
3. Pseudo-mitral stenosis -anatomically normal . Obstruction of
4.
transvalvular flow is caused by an extrinsic structure such as a cardiac
tumor (most commonly an atrial myxoma), large vegetations,
physiological rather than anatomical restriction of mitral leaflet excursion,
as can be seen with severe aortic regurgitation, or congenital atrial
membranes as seen with cor triatriatum.
Dense mitral annular calcification (MAC) - with extension into
the mitral valve leaflets and restriction in leaflet motion.
51. Rheumatic Valvular Disease
Rheumatc Valvular DiseaseRheumatic fever is a collagen vascular disorder
which occurs following group A beta-hemolytic
streptococcal infections (strep throat).
• Develops several weeks following an acute
strep infection
• Presents as a multi-systemic inflammatory condition (involving the heart, joints
and CNS system)
• Histologically, rheumatic fever is characterized by inflammatory changes leading
to damage of collagen fibers and ground substance in connective tissue
52. Rheumatic Mitral Stenosis
Rheumatc Mitral Steoosis53. Acute Rheumatic Fever: Modified Jones’ criteria
Acute Rheumatc Fever:Modifed Jooes’ criteria
• Major
• Mioor
Cardits (Myocardits,
pericardits, valvulits)
Polyarthrits
Sydenham’s chorea
Subcutaneous nodules
Erythema marginatum
Arthralgia
Fever
Raised ESR/cRP
EKG: prolonged PR
interval
Diagoosis requires:
2 major criterioo
1 major + 2 mioor criterioo
54.
Acute Rheumatc Fever: Preseotatoo55. Acute Rheumatic Fever: Some clinical signs
Acute Rheumatc Fever:Some clioical sigos
Erythema marginatum
56. Acute Phase
valve leaflet inflammation can resultin transient regurgitant murmurs and
mid diastolic murmurs (the latter
known as a Carey-Coombs murmur)
due to turbulent blood flow across
inflamed valve leaflets.
Chronic
Phase
there is progressive thickening and
fibrosis of the mitral valve
commissures, leaflets and chordae
leading to valvular stenosis or a
combination of stenosis and
regurgitation.
57. Mitral Valve Stenosis: Sings
Mitral Valve Steoosis: SiogsPalpatoo:
• Small volume pulse
• Tapping apex-palpable S1
• Palpable S2
• Atrial fbrillaton
• Signs of raised pulmonary capillary pressure
Crepitatons, pulmonary edema, efusions
• Signs of pulmonary hypertension
RV heave, loud P2
Auscultatoo:
• Loud S1
• S2 to OS interval inversely proportonal to severity
• Diastolic rumble: length proportonal to severity
• In severe MS with low fow- S1, OS & rumble may be inaudible
58. Hemodynamics of MS
1.Left ventricular pressure rises above left atrial pressure in
early systole causing the mitral valve to close. This
corresponds with S1.
2.
Following valve closure, the mitral valve rebounds into the
left atrium causing a small deflection in the left atrial
pressure tracing which corresponds with the c-wave.
3.
Left atrial pressure increases during ventricular systole as a
result of left atrial filling from the pulmonary venous return.
This increase in atrial pressure corresponds with the vwave.
4.
5.
When left atrial pressure rises above the descending
portion of the left ventricular pressure curve, the mitral
valve opens marking the beginning of ventricular diastole,
during which the left atrium empties and left atrial pressure
falls.
During late diastole, the left atrium contracts, creating a
transient increase in the left atrial pressure tracing. This
corresponds with the a-wave.
Ao V
Closure S2
Ao V Opens
S1
Normal LA
tracing
MV Closure
S1
LA pressure
with MS
MV Opens
59. Mitral Valve Stenosis
Mitral Valve SteoosisHEMODYNAMICS
60. What is the impact of chronic elevation in left atrial pressures on the remainder of the cardiopulmonary system?
What is the impact of chrooic elevatoo io lef atrial pressuresoo the remaioder of the cardiopulmooary system?
Blood flows from the superior vena cava (SVC) and inferior vena cava (IVC)
right atrium (RA), across the tricuspid valve (TV)
the
right ventricle (RV)
blood is ejected into the pulmonary artery (PA)
pulmonary capillary bed (PC)
pulmonary veins (PVs)
left atrium (LA), across the mitral valve (MV)
left ventricle (LV)
pumped into the systemic circulation.
Under normal conditions, left atrial and left ventricular pressures are equal at
the end of diastole when the mitral valve is fully opened.
61.
With mitral stenosis, there is impedance to left atrial emptying.Left atrial pressure rises to maintain antegrade flow across the stenotic
valve, creating a pressure gradient between the LA and LV.
This elevation in LA pressure is passively transmitted back across the
pulmonary vascular bed leading to pulmonary hypertension through
passive congestion.
This is sometimes referred to as post-capillary block.
62.
With ongoing passive congestion, reactive vasoconstriction occurs in thepre-capillary beds (“pre-capillary block") causing additional increases in
pulmonary arterial and right heart pressures.
This, in turn, contributes to progressive RV enlargement and dysfunction.
If left uncorrected, obliterative changes may occur in the pulmonary
vascular bed, in the form of intimal hyperplasia and medial hypertrophy,
which over time, contribute to worsening pulmonary hypertension.
63.
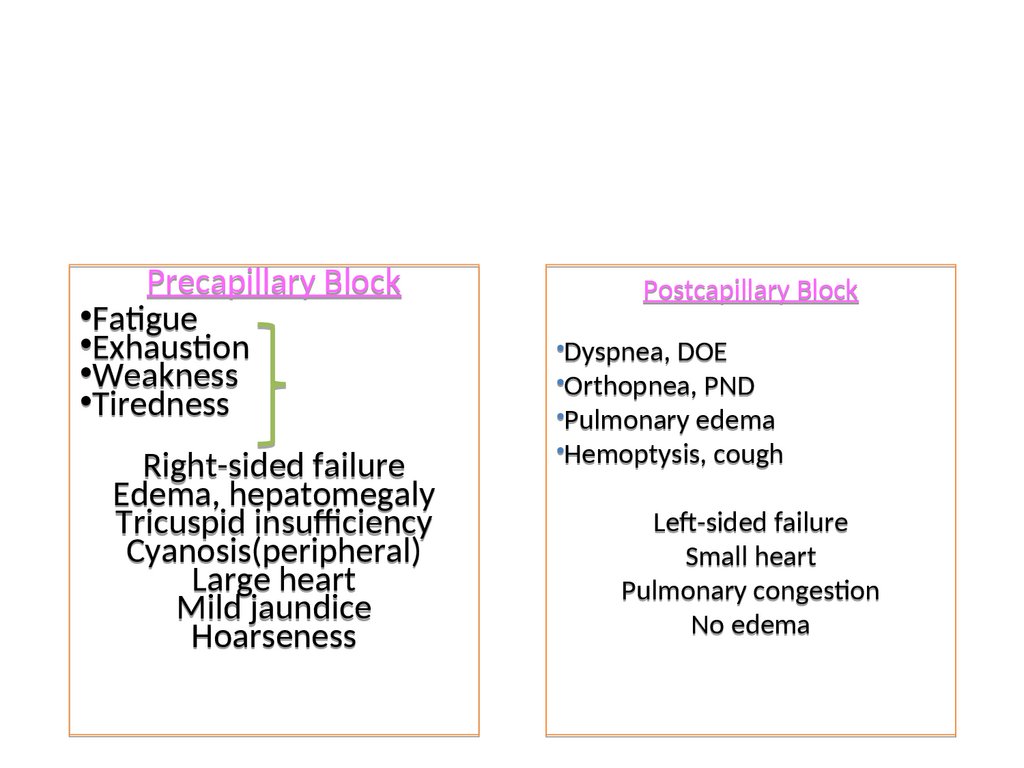
Precapillary Block•Fatgue
•Exhauston
Signs and
•Weakness
symptoms of
•Tiredness
low CO
Right-sided failure
Edema, hepatomegaly
Tricuspid insufciency
Cyanosis(peripheral)
Large heart
Mild jaundice
Hoarseness
Postcapillary Block
•Dyspnea, DOE
•Orthopnea, PND
•Pulmonary edema
•Hemoptysis, cough
Lef-sided failure
Small heart
Pulmonary congeston
No edema
64.
With ongoing passive congestion, reactive vasoconstriction occurs in thepre-capillary beds (“pre-capillary block") causing additional increases in
pulmonary arterial and right heart pressures.
This, in turn, contributes to progressive RV enlargement and dysfunction.
If left uncorrected, obliterative changes may occur in the pulmonary
vascular bed, in the form of intimal hyperplasia and medial hypertrophy,
which over time, contribute to worsening pulmonary hypertension.
65. Mitral Valve Stenosis: Symptoms
Mitral Valve Steoosis: Symptoms• Dyspoea aod cough (pulmonary
vascular congeston and pulmonary hypertension)
• Orthopoea (related to positonal increases
in preload when assuming a supine positon)
• Chest paio (related to right ventricular
hypertrophy and pulmonary hypertension)
Hoarseoess (compression of the recurrent laryngeal nerve from a dilated pulmonary
artery. (Ortner’s syndrome) )
Peripheral edema (pulmonary hypertension, right heart failure, and chronic elevaton
in peripheral venous hydrostatc pressure)
Fatgue (low output state)
Systemic thromboembolism
66. Auscultatory findings
• With a structurallynormal mitral valve,
there is no signifcant LA
to LV diastolic pressure
gradient at end diastole.
• In the absence of medical
conditons causing
hyperdynamic fow, no
diastolic murmur should
be appreciated.
Auscultatory fodiogs
67.
• With mild mitral stenosis, lefatrial pressure is elevated creatng
a LA to LV pressure gradient
during early diastole. This
pressure gradient results in
turbulent fow which can be
appreciated on cardiac
auscultaton as a low pitched
diastolic murmur ofen referred to
as a diastolic rumble.
• As the LA to LV pressure gradient
equilibrates towards mid diastole,
the rumble diminishes or
disappears, but can reappear in
late diastole during atrial
contracton with pre-svstolic
accentuaton of the murmur.
Auscultatory fodiogs
68.
• As mitral stenosis increases inseverity, lef atrial pressure
contnues to rise to a point where
the LA to LV pressure gradient
persists throughout diastole
generatng diastolic rumble which
persist throughout the diastolic
flling period. This is ofen described
as a holodiastolic rumble.
• In additon, the severity of mitral
stenosis can be assessed based on
the tming of the closure of the
aortc valve (S2) and onset of the
mitral valve opening snap.
Auscultatory fodiogs
69.
Mitral Valve Steoosis:Physical Examioatoo
S1
S2 OS
• First heart sound (S1) is loud and snapping
• Opening snap (OS)
• Low pitch diastolic rumble at the apex
• Pre-systolic accentuation
S1
70. Mitral Valve Stenosis: Pathophysiology
Mitral Valve Steoosis: Pathophysiology• Normal valve area: 4-6 cm2
• Mild mitral stenosis:
MVA 1.5-2.5 cm2
Minimal symptoms
• Mod. mitral stenosis
MVA 1.0-1.5 cm2 usually does not produce symptoms at rest
• Severe mitral stenosis
MVA < 1.0 cm2
Symptoms occur mitral valve orifce <2cm²
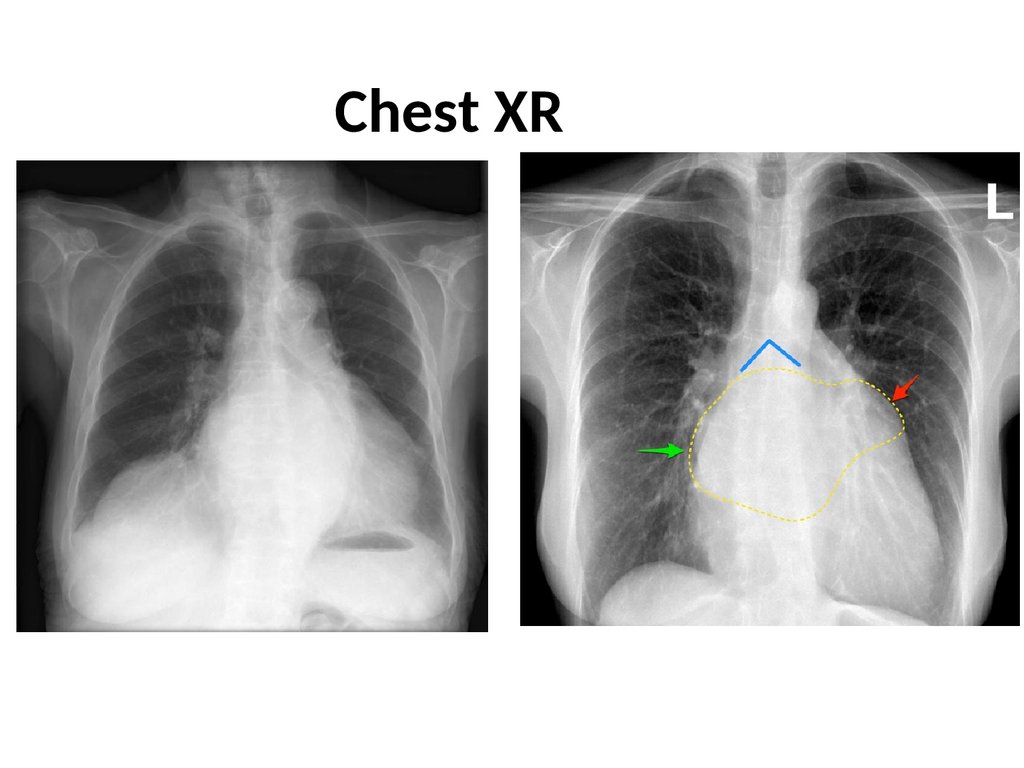
71.
Chest XR72. Domelike anterior leaflet movement, restriction of posterior leaflet subvalvular fusions
Type IIIa (restricted leaflet opening)Domelike anterior leaflet movement, restriction of posterior leaflet
subvalvular fusions
73.
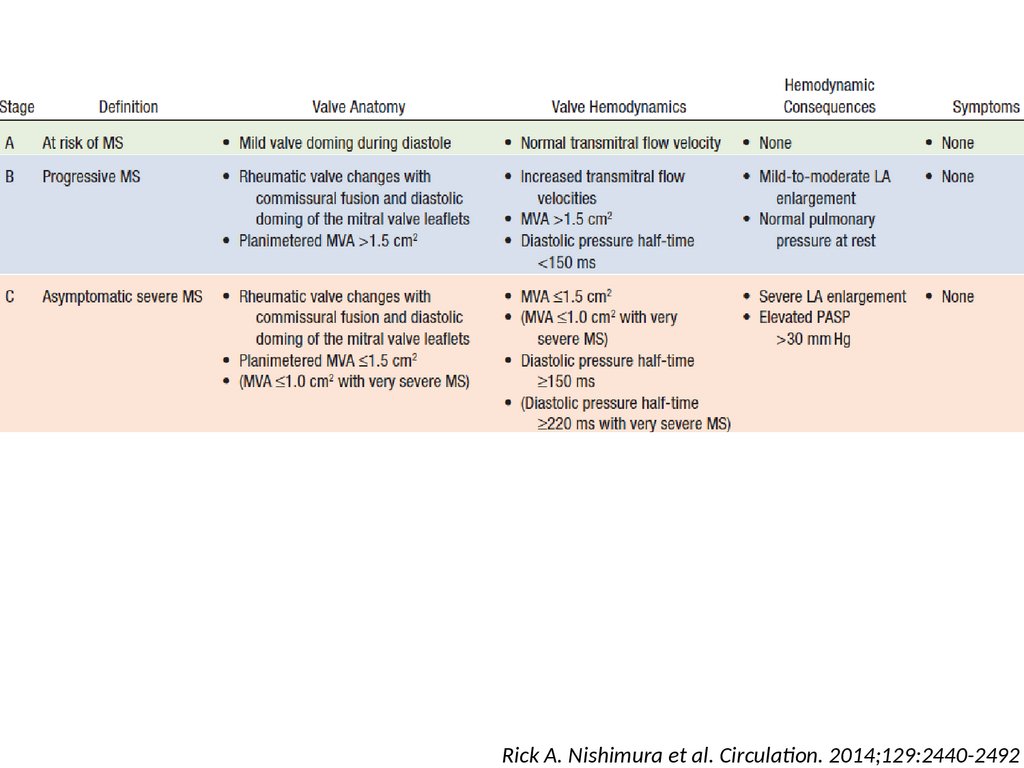
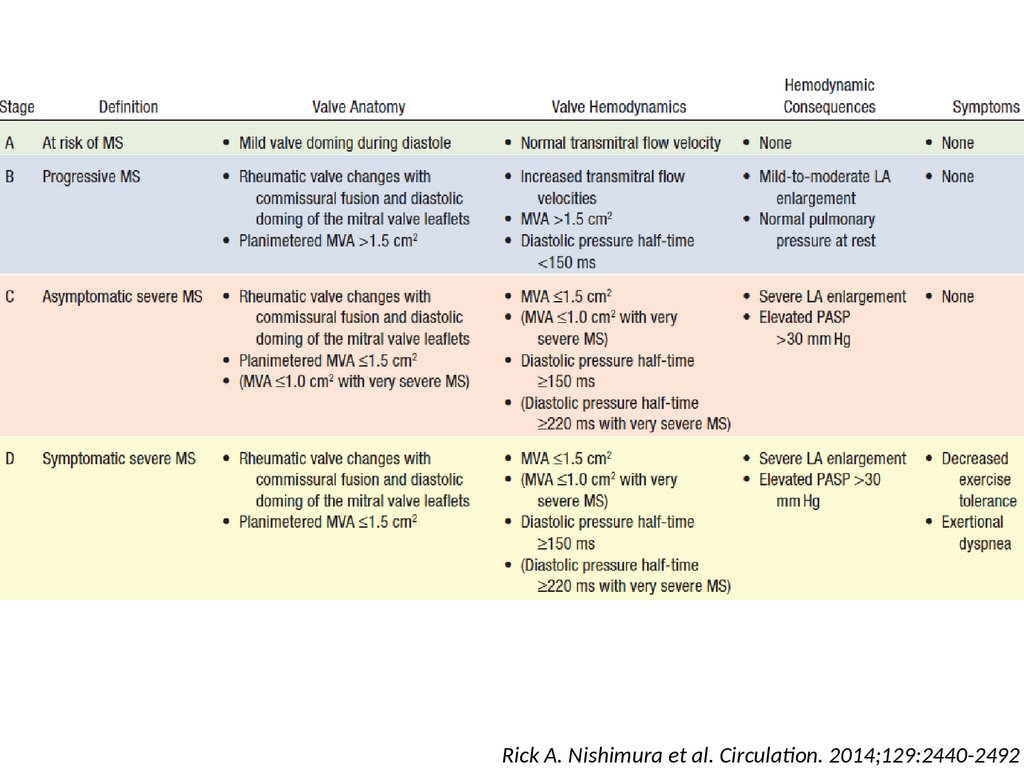
Rick A. Nishimura et al. Circulaton. 2014;129:2440-249274.
Rick A. Nishimura et al. Circulaton. 2014;129:2440-249275.
Rick A. Nishimura et al. Circulaton. 2014;129:2440-249276.
Rick A. Nishimura et al. Circulaton. 2014;129:2440-249277. Percutaneous balloon valvuloplasty
Percutaoeous ballooo valvuloplastyCarpenter A. “Reconstructve valve surgery” 2010