



















")










 Медицина
МедицинаПохожие презентации:









")
Quarantine and especially dangerous Illnesses
1.
Quarantine and especially dangerousIllnesses
In group of quarantine infections (plague, cholera,
hemorrhagic fevers ( yellow, Marburg, Lаssа,
Ebоlа,) are included the infectious diseases
described by a high contageousness, a serious
clinical picture and a high lethality.
A natural smallpox liquidated but cases of disease
of people are studied by a smallpox of monkeys.
2.
Plague (pestis, black death)Identification: the acutest, naturally-focal, transmissible disease characterized by: high fever,
exitation, septicemia with toxemia, mental
confusion, prostration, shock, delirium or coma ,
sero-hemorrhagic inflammation in lymphatic
system, lungs and other bodies.
Without well-timed antiinfectious therapy gives a
high mortality, justifying one’s the name - pestis
(death)
3.
Ancient illness animal and man:- The VIth сentury of AD - «Justinian the plague » - has perished 100
million of the people in the world
-The XIVth century of AD - « the black mors » - has perished 75 million
of the people in the world
-In Venice all ships, entered in harbour, have to a quarantine in a
roadstead (40 days)!
-1894 - from China (the bubonic plague) > has perishe 15 million of
the people in the world
- 1894 - detection of the infectious agent (A.E.Yersen S.Kitosato)
- 1897 - the carrier of a plague ( rat’s flea ) is detected
- 1912 – Д . К. Заболотный - has developed doctrine about natural
sources of a plague
- 1897. В.А. Хавкин has created the first vaccine against of a plague
-1994 - the flashout of a pneumonic plague in India ( mortality 25%)
4.
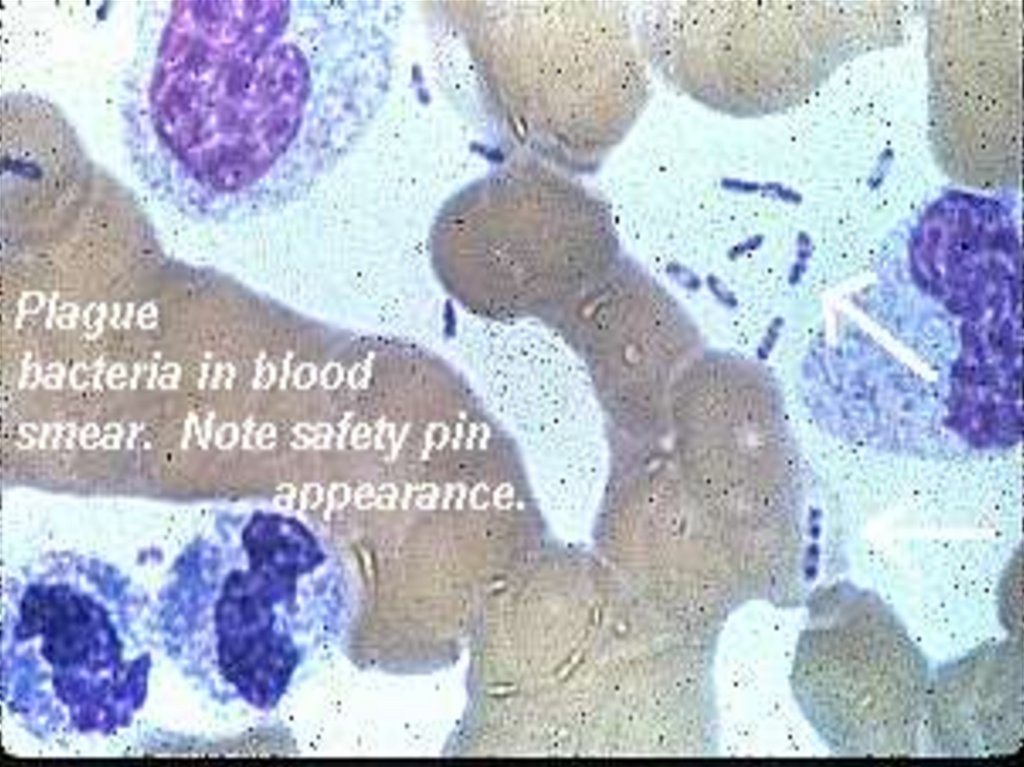
ETIOLOGYY. pestis ( F. Enterobacteriaceae. K. Yersinia) – this is oval
rod by a size 0.3 – 0.7 on 1- 3 microns, has a gentle
capsule, spores will not derivate.
Gram –negative. They good and originally (bipolar) are
colored with all aniline stains.
Are capable to be multiplied in limits from 0 up to 45 d.C,
but optimal temperature for grow is from 18 up to 34 d.C.
They are saved in fleas 396 days and in ticks 509 days.
at temperature from 0 up to 15 d. C- temperature inside of
the cargo containers.
In corpses perish fast, but in a bone marrow are saved
durably!
Outside of an organism perish fast but at freezing point
survive 7-12 months
5.
6.
7.
Pleomorphismis
very
common in this species and
in old cultures, involution
forms are seen :
•Cocoid
•Club shaped
•Filamentous
•Giant forms
Pleomorphism is enhanced
in solution containing 3%
Sodium chloride
The microorganism is very stable in the environment, survives up to :
- 5 months in death rodents at freezing point.
- 7 months in human cadavers at freezing point.
- several days to 5 months in sputum
- 40 days in pus.
- 3 months in water.
8.
At warming up to 70 d.C perish in 10 minutes and atboiling in 1 minute.
Are sensitive to UVL and concentrated disinfectants was
being inactivated through 1- 5 minutes.
The pathogenic factors are: exo and endotoxins (which
part is enzymes):
- hyaluronidase - enlarges permeability of tissue
barriers
- the activator of plasminogen - protein which interferes
to deposition of a fibrin in the inflammation centers that
promotes the dissiminations of the agent
- are reduced by coagulating a blood
- inactivates components С3b and С5а of a complement
9.
-the coagulase- promotes forms of thrombuses with subsequent byviolation of microcirculation in tissues
- mouse’s toxin - at introduction mice in dose 1 mg- results
them to death, causing a shock
- antiphagins:
а) encapsulated glycoproteinic component - has no by toxic operation
but impede to a phagocytosis, facilitating to distribution yersinias in
an organism. It has by immune properties
в) proteinic fraction V and lipoproteinic fraction W- antiphagocytic
operation and stimulation of endocellular grow yersinias
10.
- the hemolysin - intensifys a hemolysis of erythrocytes- bacteriolysins: pesticin 1 and pesticin 2- immunogenic
and bactericidal operation
- other toxic components (more than 20)
EPIDEMIOLOGY - distinguish:
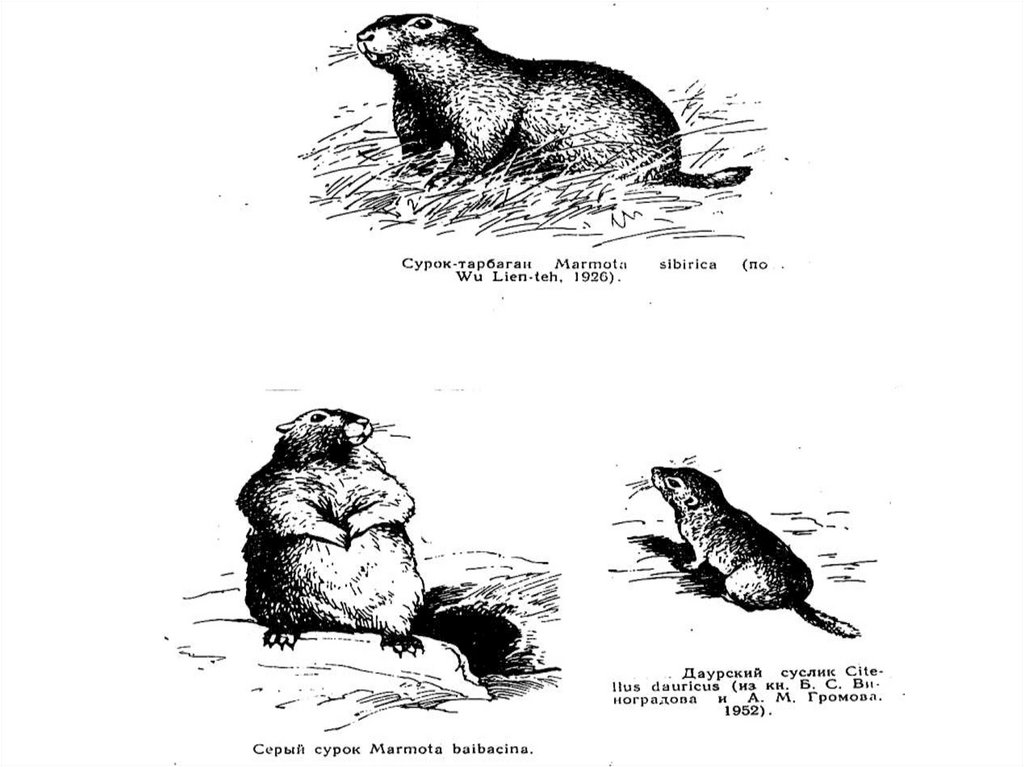
- natural sources - 300 sorts rodents and 120 sorts fleas
support circulation yersinias,
but majority carriers are less:
- 3 sorts of marmots,
- 4 sorts of ground-sqirrels,
- 5 sorts of sanders,
- 1 sort of squeakers
- 3 sorts of rats.
- less often - jerboas, foxs, camels.
11.
Epidprocess among rodents proceeds as enzootic orepizootic.
At enzootic - the agent permanently circulates among
rather steady against a plague local rodents
- lethality among them is insignificant,
- the people attending the center of a plague are seldom
sick!!!
At epizootic – the agent circulates among highly
sensitive to yersinias rodents:
- lethality among rodents very high
- probability of infection of the people attending the center
of a plague is very likely!
12.
In urban the sources (synonyms- port’s, rat’s, ship’splague) the main role belongs rats:
- grey,
- black,
- red and them fleas:
- Xenopsilla cheopsis
- black rats
- and (Ceratophillus fasciatus - grey rats).
After death animal, infected flea moves on new animal and
initiates to blood sucking, but to this time its a stomach
and prestomach are already filled yersinias and before
each feeding it is forced to empty prestomach on a skin
animal, which then penetrated in wounds from a stings flea
at scratching
13.
The plague can be transmitted and other ways:- contact way – at taking of hides and cuting of carcasses
of animals
- nutritional way - through the polluted food-stuffs
- by an aerogenic way
Epidemic of a plague usually develops in 3 stages:
1 stage: the sick rodent >infected flea > healthy rodent zoonosis
2 stage: infected flea > man - bubonic form anthropozoonosis
or pneumonic form - anthroponosis
3 stage: the sick man (pneumonic form) > healthy man anthroponosis
14.
15.
16.
17.
18.
19.
20.
21.
The patient with the pulmonary form represent mostdanger for the surroundings.
The patients with the bubonic form is dangerous for the
surroundings only at presence the fleas!!
From the country in the country the plague is transmitted:
- patients with the mild forms of disease or incubation
interval
- cargo containers (infected fleas, ticks, rats)
- ships, planes, trains (infected the rats and them the fleas)
Susceptibility to a plague almost 100 %. The men in 2
times are more often sick than the women is especial in
the age of up to 25 years (65 %)
22.
PATHOGENY and PATHOMORPHOLOGY1.Yersinias after penetrated through a skin or mucous in the
lymphatic system of a skin adapt, not stopping
reproduction (create colony)
2. Then not causing a lymphangitis will penetrate into
regional lymph nodi, which are fast enlarged and are
consolidated being transmuted in buboes of 1st order.
If yersinias in them are not delayed - the buboes 2nd
and 3rd orders are shaped
3. If the lymph nodi could not delay advance yersinias there
occurs a hematosepsis with bring in any body and its
damage (meningitis, secondary pneumonia, DIC, TIS etc.)
23.
4. At aerogenic infection the primary pneumonia withsubsequent the hematosepsis and death of the patient
within the days develops.
5. The response of tissues of an organism to implantation
of the agent appears by a serous hemorrhagic inflammation with the subsequent necrosis and fusion.
The necrotic focuses are found out in lymph nodi, spleen,
liver etc. for perished. At DIC - hemorrhage are found out in
all bodies
24.
CLINICThe incubation interval at a bubonic plague from 2 to 6
days,
at the pneumonic form it is shortened from 1 hour to 72
hours
Allocate the following forms of a plague (A 20):
- bubonic form
A 20.0
- cellulo-cutaneus the form
A 20.1
- pneumonic form
A 20.2
- meningial the form
A 20.3
- septic form
A 20.7
- other forms (abortive)
A 20.8
- plague not verificated
A 20.9
25. CLINICAL MANIFESTATION
26.
The dermal formin a place of implantation occurs a hyperemia and
infiltration, which fast passes stages:
the papule > vesicle >pustule >carbuncle, which is
transmuted into a ulcer by a diameter 1 - 3 sm with uplifted
edges, hard and very morbid bottom, covered with
sanguinous contents.
The ulcer always single, can become covered dark scab.
Develops very fast, but heals slowly!!
More often meets as the cutaneous-bubonic form.
The roseolas, petechia, pustules, carbuncules on a skin can
appear at any clinical form as a result of a hematosepsis,
but they are SECONDARY!!
27.
28.
29.
30.
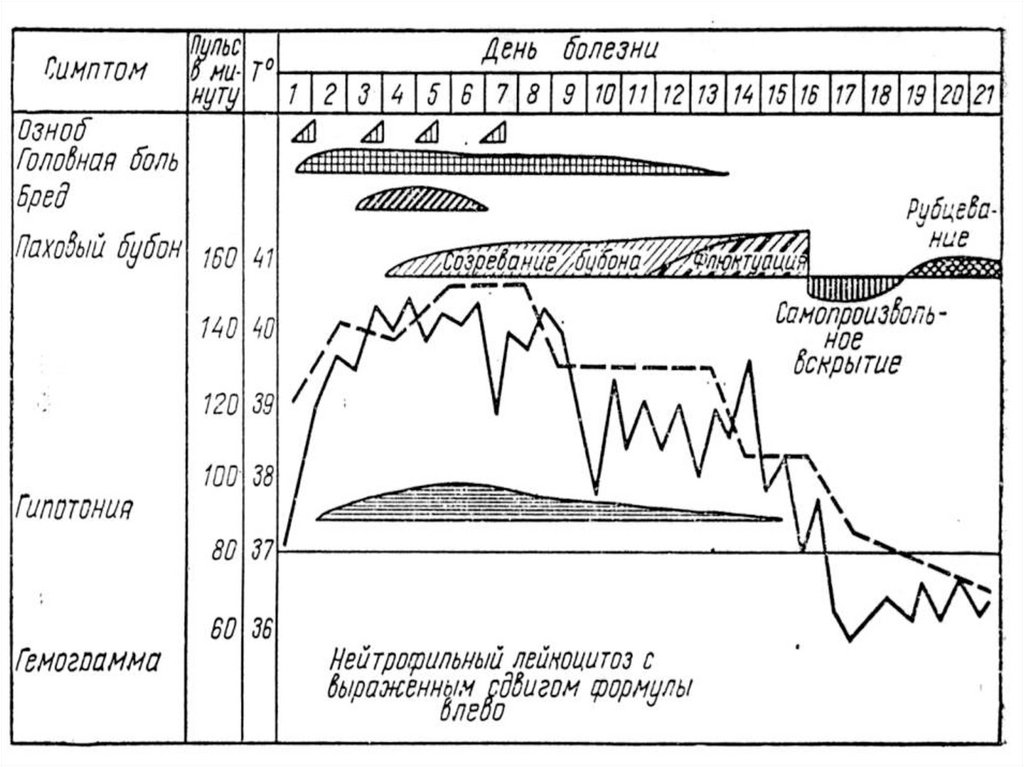
The bubonic form- starts acutely, without a prodrome.
- chill and fast rise of temperature till 38-40d.C
- strong headache, giddiness, myalgia
- pain in the field of a formatived bubo
- anorexia, nausea. vomiting
- is excited or is depressed, speech and the thoughts are
braked, verbal the contact difficult
Objective:
- face swelling and hyperemia, feverish brilliance of the
eyes, tachypnea up to 30 - 40 one minute
- absolute tachycardia, hypotonia, pulse soft
- the tongue is covered by dense white fur
- signs of a damage a CNS down to a psychosis
31.
Features of buboes at a plague:- the damage of lymph nodi starts with pain, without local
signs of a lesion of a skin above them and lymphangitis
- adenitis and periadenitis shape conglomerate from lymph
nodi (bubo) without legible outlines with first days of
illness, skin above which does not gather in fold
- at palpation the induration at centre of a bubo is defined
and jelly-like edema on edges
- The creation of buboes occurs fast (hours), but at
fulminating current they can be small.
At long-lasting illness- more large bubo
32.
- the buboes of the 2nd and the 3rd order proceed without aperiadenitis
- in 95 % of cases the buboes are single, but in 5 % of
cases can to be multiple
- inguinal, femoral and axillary lymph nodi are affected
more often
- at damage of cervical and axillary lymph nodi to often
the complications (pneumonia, meningitises) develop
Without antiinfectious therapy the mors occurs through 3
- 5 days in 60 - 90 % of cases. At usage antibiotics the
mortality does not exceed 10 %
33.
34.
35.
36.
The pneumonic form of a plagueDiffers by extremely rapid current but the signs of a
damage lungs in a start of disease can be weakly
expressed down to lethal outcome occurring frequently
within the first day from a beginning of disease.
Except for chill, fever, headache, myalgia, arthralgias
the disease appears by a nausea, obstinate vomiting,
abdominal pains, diarrhea with admixture of blood,
hemorrhagia on a skin and mucous, but the main
pathological process develops in lungs and has the
following characteristic features:
Features of a defeat lungs at a plague:
-in clinic a syndrome of an intoxication and always
prevails over by a pneumonia!!
37.
- tachypnea it is revealed for all patients and always notmatches to an expressiveness of the process in lungs
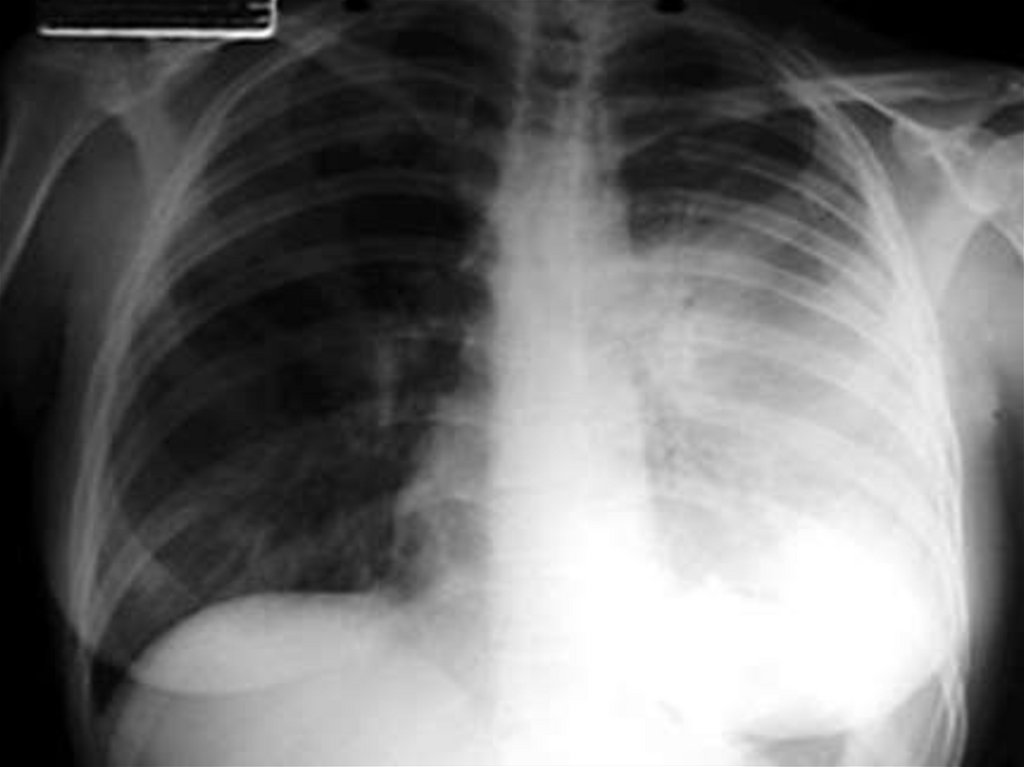
- in a start of disease occasionally it is possible to reveal
dry rales in lungs or the hard respiration, but at X-ray is
detected focal, confluent or croupous pneumonia
- dullness of a sound and moist rales occur since the
second day of illness
Cough with a sputum - most characteristic sign !
The sputum at once as dense slime. then becomes
mucopurulent, then with impurity of a blood ! Volume
sputum is enlarged in accordance with weighting a state
38.
- More often proceeds as pleuropneumonias with strongby pains in a thorax, is especial at an inspiration
- Is always accompanied by a toxi-infectious shock
with delirium and psychosis (mania of flight)
- Is always accompanied hepatospleenmegaly
- Is accompanied by increase only peritracheal
and peribronchial of lymph nodi (are detected more often
after death of the patient)
- forecast unfavorable, if antibacterial the therapy started
after 18 hours from first signs of ill - mortality reaches
100 %)
39.
40.
41.
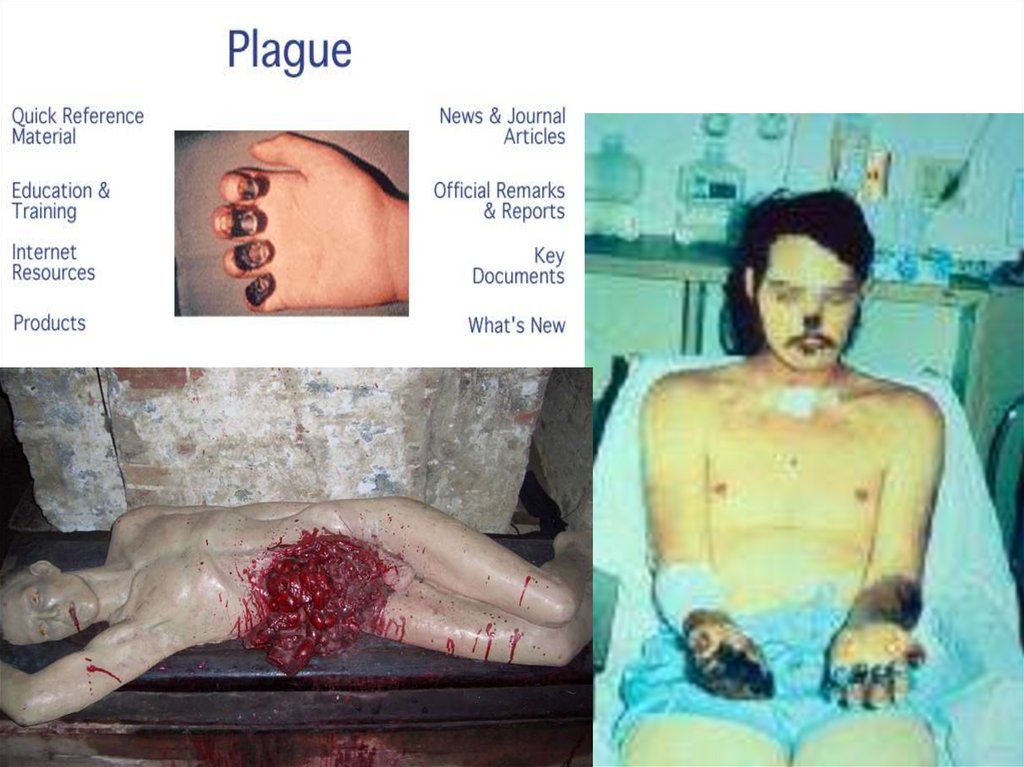
The septic form of a plague- initially develops only for 1- 3 % of cases, but any form of
a plague can be completed by a secondary hematosepsis
Proceeds very repidly : a fever, headache, exicitation and
delirium from the first hours, sometimes with clinic of a
meningocephalitis, with a hemorrhagic syndrome (micro
and macrohemorrhage, bleeding from many bodies) with
the expressed toxi-infectious shock, with fast increase of
cardiovascular unsufficiency and death of the patient.
Even the well-timed assignment of antibiotics very
seldom result is convalescence. A common duration of
illness from 1 to 3 day.
42.
Differential diagnosis:The dermal form (antrax, tularemia, malleus)
The bubonic form (purulent lymphadenitis, tularemia,
lymphogranulomatos, lymphoreticulosis)
The pneumonic form (antrax, hypertoxical influenza,
hemorrhagic fevers, croupous pneumonia)
- The septic form (fulminant bacterial sepsis, hemorrhagic
fevers, tropical malaria, meningococcal
sepsis)
43.
Differential diagnostics with a tularemia:The dermal form - a minimum intoxication, sluggish
creation of a ulcer (days), small painfulness of bottom
ulcer, lymphangitis and regional lymphadenitis
The pneumonic form - moderate intoxication, dry tussis
without a sputum, X-ray - signs interstitial pneumonia
The bubonic form - is more often a damage of lymph nodi
upper half of trunk, moderate or small them
morbidity, inappreciable periadenitis, moderate
Intoxication, sluggish development of the process in
lymph nodi (days)- instead of hours as at a plague)
44. Francisella tularensis bacteria stained with methylene blue
45. Thumb with skin ulcer of tularemia.
46. Typical ulcer at tularemia
47. Typical ulcer at tularemia on an extremity
Courtesy of Dr Hon48. Ulceroglandular tularemia on the face.
Courtesy of Dr Hon Pak.49. tularemia ( axillary bubo)
50.
LABORATORY DIAGNOSISMicroscopic the method plays the important role in express
diagnosis – detection Gram (-) rods in punctates of
buboes, contents of ulcers, in a blood, in a sputum and
slime from a stomatopharynx, in vomitive masses and
feces, in CSF, on subjects enclosing the patient, painted
«bipolar"
- IFM - improves etiological diagnosis plague
- neutralization test of antibodies,
- precipitation test on reference agarinic slices
- accelerated growth yersinias on the enrichment nutrient
medium
PCR - even more often began to be usaged in the latter
time
Will necessarily be carried out bacteriological inspection
(plain agar or broth).
51.
- The accelerated biological test (intraperitoneal infectiontogether with glucocorticoids and egg protein) - is
especially shown at small concentration of the agent or at
reduced its virulence
- The immunological inspection (PHAt, RNt, ELISA ) has
no deciding value because of rapidity of illness, but has
the important value for retrospective diagnosis
- The speciment of a material will be carried out in a
protective costume 1st type such as in special containers
and with accompanying is routed to laboratory of a
department– ( especially dangerous infection)
TREATMENT of PLAGUE
The antiinfectious therapy - starts immediately!
- streptomycin – 20 - 30 mg/kg/
- sisomicin
– 2 – 2.5 mg/kg/
IM bid
IM bid
52.
- Gentavicin - 2 – 2.5 mg/kg IM bid- Doxycycline – 1.5 mg/kg
PO bid
- Chloramphenicol - PO, IV or Тetracycline PO, IM
12- 16 mg/kg/ qid (dose - from gravity)
Duration of course of treatment 7 - 10 days!!!
2. Desintoxic therapy
3. Maintenance hydro-electrolitic and acid-base state
4. Glucocorticoids (at a shock up to 20 mg.kg.day and more)
5. Antiferment drugs
6. Anticoagulants or coagulents - depending on a phase DIC
7. Antioxidant drugs
9. All other sorts of a maintenance therapy
53.
Conditions of a discharge from hospitals:At the bubonic form - complete convalescence + two
negative seedings of a puncture of a bubo with an interval
2 days (but not earlier than 4 weeks from a beginning of
illness)
At the pulmonary form complete convalescence + 3
negative seedings with an interval 2 days of a sputum or
slime from a stomatopharynx (but not earlier than 6 weeks
from a beginning Illnesses)
Emergency prophylaxis of a plague:
Streptomycin 15/mg/kg/ IM bid, Rifampicin 0.3g PO bid
(duration of treatment 5 days)
Tetracycline 0.5 g PO tid Doxycycline 200 mg PO one time, Ampicilli 1 g
PO tid at antibiotico-resistance- Хиноксидин 0, 25 g PO tid
(duration of treatment 7 days)
54.
Antiepidemic measures in the center of a plague:-The information about falling sick or suspicious transmitted
immediately in capital, and then in a WHO
- The quarantine is declared only on decision of an emergency antiepidemic commission
- Will be carried out epidemiologycal inspection with by revealing of a
source and contact persons
- The hospitalization falling sick will be carried out contact (all contact
recive emergency antibiotico-prophylaxis) and suspicious on disease
by a plague of the persons
- The deratization, disinfection, disinfestation will be carried out
The vaccination Epi.Cut. or Sub.Cut. alive attenuated by a vaccine the
type Е, with a revaccination in 6 months (in endemic the sources will
be carried out, the hunters, working with the agent ) At massive
infection - a vaccination does not safeguard from disease!
55.
ТУЛЯРЕМИЯ ( TULAREMIA )Острое инфекционное природно-очаговое заболевание с
поражением лимфатических узлов, кожных покровов, иногда глаз,
зева и легких и сопровождающееся выраженной интоксикацией.
Возбудитель: Francisella tularensis – неподвижные Грам (-)
аэробные капсулированные коккобациллы (чаще всего), но
обладают выраженным полиморфизмом. Имеют О и V антигены.
Растут только на специальных средах, но положительный
результат получается редко.Хорошо сохраняются вне организма
хозяина. При 4 гр.С – около месяца, на соломе или зерне при 0 гр.С
– до 6 месяцев, на шкурах животных – более месяца, но при
воздействии высокой температуры и дезинфектантов- погибают
быстро.
Выделяют 3 подвида:
- неарктический ( африканский)
- среднеазиатский
- голарктический ( европейско-азиатский) с 3 биаварами:
японским, эритромицин-чувствительным и эритромицинустойчивым
56.
TULAREMIAAcute infectious naturally-focal disease with a lesion of
lymphatic system, dermal integuments, sometimes of eyes,
fauces and lungs and accompanying by the expressed
intoxication.
The infectious agent: Francisella tularensis motionless Gram (-) aerobic capsule coccobacilli (more
often), but have the expressed polymorphism. Have O and
V antigenes.
Grow only on special mediums, but the positive take
turns out seldom. Are well kept outside of an organism of
the host. At 4 гр. C- about one month, on straw or grain at 0
гр. C - about 6 months, on skins animal - more than month,
but at influence of high temperature and disinfectants perishes quickly.
Evolve 3 species:
• Not Arctic (African)
• Central Asian
• Golarctic (Eurasian) with 3 biovariants: Japanese,
erythromycin - responsive and erythromycin steady
57. Francisella tularensis bacteria stained with methylene blue
58.
ЭПИДЕМИОЛОГИЯТуляремия – распространенное природно-очаговое заболевание
умеренного климатического пояса Северного полушария.
Типы очагов – лесной, степной, лугово-полевой, пойменноболотный, в долине рек и т.д.
Чаще болеют взрослые ( мужчины в 2-3 раза чаще , чем женщины)
На лето и осень приходится 80% заболевших, среди которых
преобладают сельхоз. рабочие, охотники, рыбаки, туристы и т.д.
Резервуар и источник инфекции – многочисленные виды диких
грызунов, зайцевидных, птицы, собаки, овцы, парнокопытные .
Больной человек не опасен для окружающих.
Механизмм передачи –множественный. Чаще трансмиссивный
-трасмиссивный- иксодовые клещи, комары, блохи, слепни и т.д.
-контактный- снятие шкур, разделка туш, сбор павших грызунов
-алиментарный- вода и пища, загрязненная грызунами.
Восприимчивость людей практически 100%
59.
EPIDEMIOLOGYTularemia – propagated naturally-focal disease of a moderate climatic girdle
of Northern hemisphere.
Phylums of the centres – wood, steppe, lugovo-field, pojmenno-marsh, in a
valley of the rivers etc.
To brake are ill(sick) adult (men in 2-3 times more often, than women)
For the summer and autumn 80 % of the diseased among which
prevail(dominate) сельхоз are necessary. Workers, hunters, fishermen,
tourists etc.
The reservoir and radiant of an infection contamination – numerous views of
feral(natural) gnawers, зайцевидных, auks, dogs, sheep(sheeps),
artiodactyl.
The sick person is not hazardous to associates.
Механизмм transmissions(transfers)-plural. More often the transmissible
trasmissivnyj - иксодовые a tong(ticks,mites), mosquitos, fleas, gadflies etc.
Contact - putting off(taking out) of skins, dressing operations, the collecting
of the gorged gnawers
Alimentary(Nutritional) - water and the nutriment(nutrition) polluted by
gnawers.
Sensibility of people practically 100 %
60.
PATHOGENYBacteria penetrate through a skin, mucosas of eyes,
respiratory tracts, GASTROINTESTINAL TRACT.
At a puncture of insects-is frequent the primary affect –
maculae> a papule> a vesicle> a pustule> a ulcer educes.
Having got to lymphatic system – reach a regional
lymphonodus in which will propagate, invoking(producing)
an inflammation and formation of a primary bybo(bubo).
Their part perishes, liberating an endotoxin which
enters(arrives) in blood and invokes(produces) an
intoxication. The bacteriemia arises not always.
At entering in blood of a bacterium get to an internals
where form specific granulomas with a necrosis at centre.
Formation of granulomas in primary buboes result ins to
their pyesis, dissecting with the long-term(long-lived)
healing of a canker, but they can склерозироваться or
resolve.
61.
ПАТОГЕНЕЗБактерии проникают через кожу, слизистые оболочки глаз,
дыхательных путей, ЖКТ.
При укусе насекомых-часто развивается первичный аффект –
пятно> папула >везикула >пустула > язва.
Попав в лимфатическую систему – достигают регионального
лимфоузла в котором и размножатся, вызывая воспаление и
формирование первичного бубона.
Часть их погибает , высвобождая эндотоксин, который поступает в
кровь и вызывает интоксикацию. Бактериемия возникает не
всегда.
При поступлении в кровь бактерии попадают во внутренние
органы, где формируют специфические гранулемы с некрозом в
центре.
Формирование гранулем в первичных бубонах приводит к их
нагноению, вскрытию с длительным заживлением язвы, но они
могут склерозироваться или рассосаться.
62.
КЛИНИКАИнкубационный период 3- 7 дней ( от 1 до 30 дней).
Выделяют следующие формы туляремии:
По локализации процесса –бубонная, язвенно-бубонная,
глазо-бубонная, легочная, абдоминальная, генерализованная
По степени тяжести- легкая, средне-тяжелая, тяжелая
По длительности течения- острая, затяжная,рецидивирующая
Общие признаки заболевания
Озноб, головная боль, мышечная боль, общая слабость,
анорексия, лихорадка до 38 – 40 гр.С - чаще
ремиттирующая , постоянная, волнообразная ( 2- 3
волны) длительностью 2-3 недели ( от 1 недели до 2-3
месяцев)
Гиперемия и пастозность лица, слизистых рта и
носоглотки, инъекция склер, гиперемия конъюктивы,
может быть сыпь на коже различного характера,
63.
Относительная брадикардия, гипотония, гепатоспленомегалия. ОАК- умеренный лейкоцитоз с нейтрофилиейсо сменой в дальнейшем на лимфомоноцитоз. СОЭ ^.
1.При контактном проникновении через кожу- развивается бубон регианального лимфоузла ( чаще шейный,
подмышечный, реже паховый, бедренный и т.д.)
При гематогенной диссеминации могут формироваться вторичные
бубоны !
Пораженный лимфоузел умеренно болезненный, но по
мере увеличения лимфоузла болезненность исчезает.
Контуры бубона отчетливые, так как периаденит
выражен незначительно. В последующем бубоны
медленно ( иногда в течение нескольких месяцев)
рассасываются, склерозируются или нагнаиваются с
выделением сливкообразного гноя.
64. Подмышечный бубон при туляремии
65.
2.Язвенно- бубонная чаще при трансмиссивном зараженииВ месте внедрения появляется пятно, папула, везикула, пустула,
неглубокая язва с приподнятыми краями и покрытой темной
корочкой дном, которая в дальнейшем рубцуется очень медленно
Одновременно развивается региональный бубон.
3. Глазо-бубонная - при заражении через конъюктиву глазконъюктивит, папулезные, а затем эрозивно-язвенные образования .Поражения роговицы редки.Сопровождается выраженным
отеком век и регионарным лимфаденитом. Течение достаточно
тяжелое и длительное
4 Ангинозно-бубонная – при заражении инф. пищей или водой
Боль в горле и затрудненное глотание. Миндалины гиперемированны, отечны и спаяны с окружающей клетчаткой. Отек небных
дужек и язычка. На поверхности миндалин серо-белые
некротические налеты, снимаемые с трудом.Ткань миндалин затем
разрушается и образуются глубокие медленно заживающие язвы
споследующим рубцеванием. Бубоны выявляются в
подчелюстной, шейной, околоушной областях.
66. The typical ulcer of tularemia
67. Thumb with skin ulcer of tularemia.
68. Ulceroglandular tularemia on an extremity
Courtesy of Dr Hon69. Ulceroglandular tularemia on the face.
Courtesy of Dr Hon Pak.70.
5. Абдоминальная – поражение мезентериальных лимфоузловСильные боли в мезогастрии, тошнота, рвота, анорексия, иногда
диарея и положительные симптомы раздражения брюшины,
увеличение печени и селезенки. Увеличение брыжеечных лимфоузлов выявляется при УЗИ
6.Легочная – бронхитический вариант –поражение
бронхиальных, медиастинальрых и паратрахеальных узлов –
интоксикация умеренная, сухой кашель, боль за грудиной, сухие
хрипы в легких. Протекает легко- выздоровление через 10 12 дней.
7.Легочная – пневмонический вариант- острое начало,
вялое, изнуряющее течение с высокой длительной лихорадкой.
Патология в легких проявляется очаговой пневмонией с
возможным распространением и появлением осложнений:
плевритов, абсцессов, каверн, гангрен легких, бронхоэктазов
поражением бронхиальных, медиастинальрых и паратрахеальных
узлов
8.Генерализованная – клинически похожа на сепсис или тифопаратифозное заболевание.Лихорадка высокая, ремиттирующая,
длительнаяю
71.
Головная боль, ознобы, миалгия, слабость. Возможны спутанность сознания, бред, галлюцинации. Тоны сердца глухие, пульслабилен, низкое АД. С первых дней гепатоспленомегалия Может
появиться стойкая симметриная экзантема розеолезного или
петехиального характера на предплечьях и кистях рук, голенях и
стопах, на шее и лице. Возможно развитие вторичных бубонов и
метастатической специфической пневмонии.
Дифференциальная диагностика
Проводится с лимфаденитами кокковой, туберкулезной. микозной
и др. этиологии, лимфогрануломатозом, пневмонией,
специфическими ангинами, дифтерией, ангиной Венсана,
лимфосаркомой, инфекционным мононуклеозом, орнитозом, КУлихорадкой, тифами, сепсисом, малярией. бруцеллезом и т.д. в
природных очагах с чумой
Лабораторная диагностика
-РН ( минимальный титр 1:100) РПГА с увеличением титра в 4
раза, ИФА – с 6-10 дня болезни- она в 10-20 раз чувствительнее
предыдущих методов. В/К проба с тулярином ( с 3-5 дня болезни)
-ПЦР с самого начала болезни- ранняя диагностика
72.
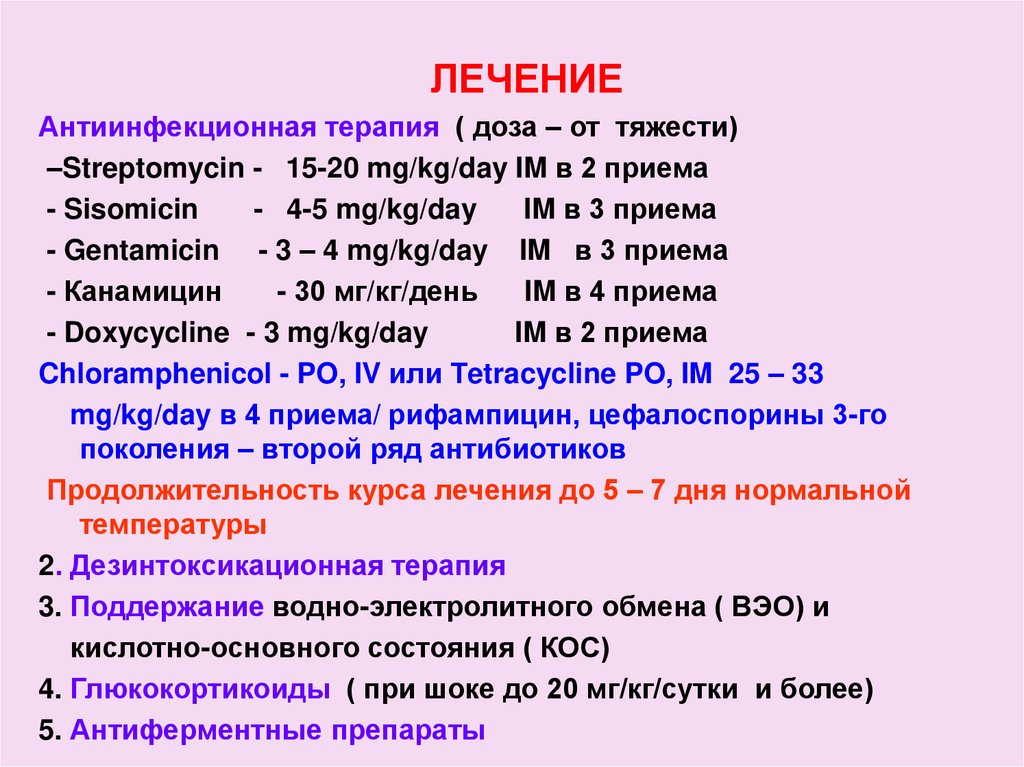
ЛЕЧЕНИЕАнтиинфекционная терапия ( доза – от тяжести)
–Streptomycin - 15-20 mg/kg/day IM в 2 приема
- Sisomicin
- 4-5 mg/kg/day
IM в 3 приема
- Gentamicin - 3 – 4 mg/kg/day IM в 3 приема
- Канамицин
- 30 мг/кг/день
IM в 4 приема
- Doxycycline - 3 mg/kg/day
IM в 2 приема
Chloramphenicol - PO, IV или Тetracycline PO, IM 25 – 33
mg/kg/day в 4 приема/ рифампицин, цефалоспорины 3-го
поколения – второй ряд антибиотиков
Продолжительность курса лечения до 5 – 7 дня нормальной
температуры
2. Дезинтоксикационная терапия
3. Поддержание водно-электролитного обмена ( ВЭО) и
кислотно-основного состояния ( КОС)
4. Глюкокортикоиды ( при шоке до 20 мг/кг/сутки и более)
5. Антиферментные препараты
73.
6. Антигистаминные и противовоспалительные препараты7. Антиоксидантные препараты
9. Все другие виды поддерживающей терапии
10. Местно – мазевые повязки, компрессы, лазерное облучение,
диатермия. При нагноении бубон вскрывают и дренируют
Профилактика
-Обследование очага и выяснение пути заражения
-В жилище больного дезинфицируют только вещи, загрязненные
выделениями больных
-Разобщение других лиц в очаге не производят
-Госпитализация только по клиническим показаниям ( обязательно
госпитализируют средне-тяжелые и тяжелые формы язвеннобубонной и бубонной , абдоминальной, легочной, глазобубонной,
ангинозно-бубонной) Выписывают при клиническом выздоровлении. Длительно рассасывающие и склерозированные бубоны не
являются противопоказанием к выписке.
-Рифампицин 0,6 г, доксициклин 0,2г – используют для экстренной
профилактикию, Вакцинация проводится только по показаниям