")


























 Медицина
МедицинаПохожие презентации:










Schistosomiasis (bilharziasis)
1. Schistosomiasis (bilharziasis)
2. Schistosomiasis - infectious diseases caused by a group of tropical parasites with a primary lesion of urogenital organs and
digestive system.The World Health Organization (WHO) estimates
that 200 million people are infected and 120 million
display symptoms. Another 600 million people are at
risk of infection.
In fact, only malaria accounts for more diseases than
schistosomiasis.
3.
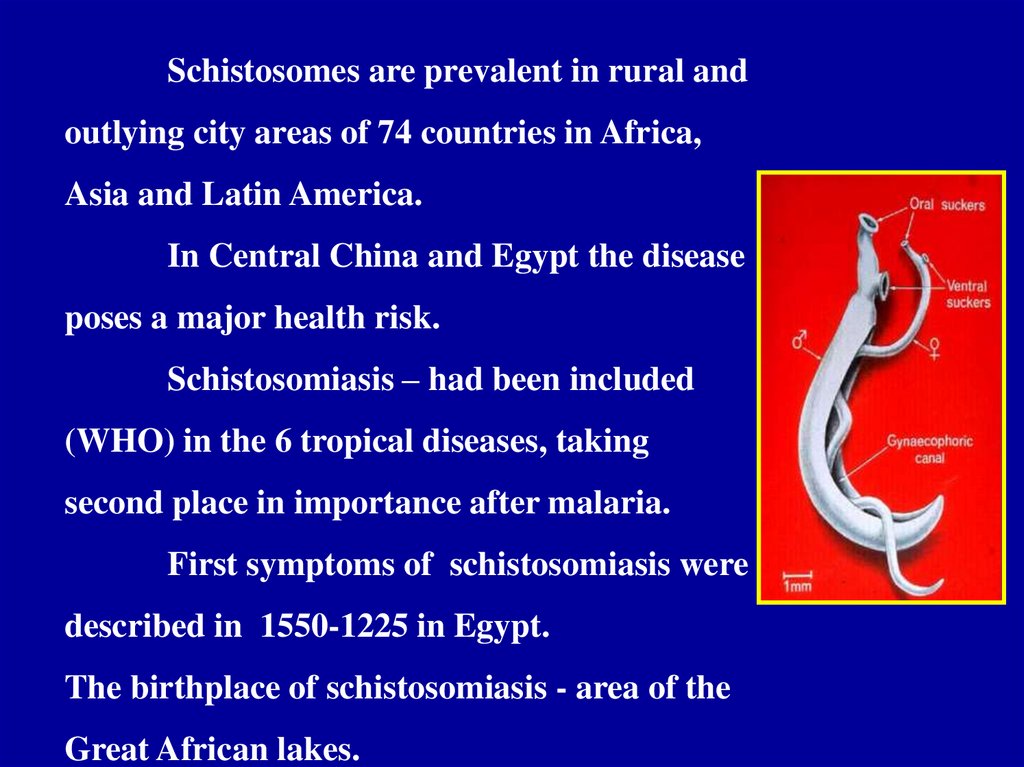
Schistosomes are prevalent in rural andoutlying city areas of 74 countries in Africa,
Asia and Latin America.
In Central China and Egypt the disease
poses a major health risk.
Schistosomiasis – had been included
(WHO) in the 6 tropical diseases, taking
second place in importance after malaria.
First symptoms of schistosomiasis were
described in 1550-1225 in Egypt.
The birthplace of schistosomiasis - area of the
Great African lakes.
4.
It is difficult to know how many individuals die ofschistomiasis each year because death certificates and
patient records seldom identify schistosomiasis as the
primary cause of death. Mortality estimates vary related to
the type of schistosome infection but is generally low, for
example, 2.4 of 100,000 die each year from infection with S.
mansoni.
5. 1851 - Bilharz opened pathogen of urinary schistosomiasis. 1898 - Manson described the causative agent of intestinal
schistosomiasis.1904 - Katsurada in Japan have found the pathogen of urinary
schistosomiasis.
Area of distribution - between 38 degrees of North latitude
and 35 degrees of South latitude.
Class - Тrematoda
Family - Schistosomatidae
Genus - Schistosoma
There are five species of
schistosomes that are prevalent
in different areas of the world
and produce somewhat
different symptoms:
6.
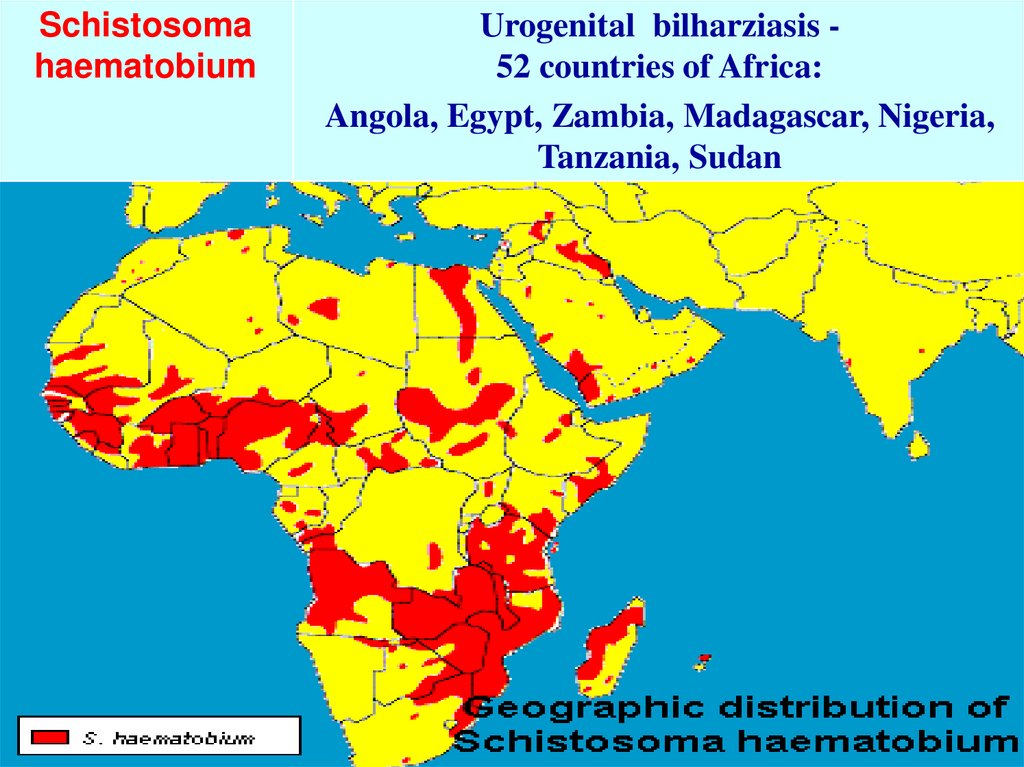
Schistosomahaematobium
Urogenital bilharziasis 52 countries of Africa:
Angola, Egypt, Zambia, Madagascar, Nigeria,
Tanzania, Sudan
7.
Schistosoma.mansoni
Schistosoma
intercalatum
Intestinal Manson’s bilharziasis
Schistosoma mansoni is widespread in 53
countries of Africa (Cameroon, Gabon, Zaire,
Congo, Chad), Eastern-Mediterranean, the
Caribbean, and South America and can only
infect humans and rodents.
8.
Schistosomajaponicum
S. mekongi
Japanese (Katayama fever)
- is limited to China and the Philippines and can infect
other mammals, in addition to humans, such as pigs, dogs
and water buffalos.
- is prevalent only in the Mekong river basin in Asia.
9.
Intestinal schistosomiasis, caused by Schistosoma japonicum,S. mekongi, S. mansoni, and S. intercalatum can lead to serious
complications of the liver and spleen.
Urinary schistosomiasis is caused by S. haematobium.
10.
Source of the infection:S. mansoni, and S. intercalatum human, rats, monkey
S. mekongi – man, dog
Schistosoma japonicum – man, home
and wild animals, large and small
cattle.
All five species are transmitted
by the same mechanism – percutaneous
- through direct contact with fresh
water infeсted with the free-living form
of the parasite known as cercariae.
Building of dams, irrigation systems, reservoirs and the movements
of refugee groups introduce and spread schistosomiasis.
11.
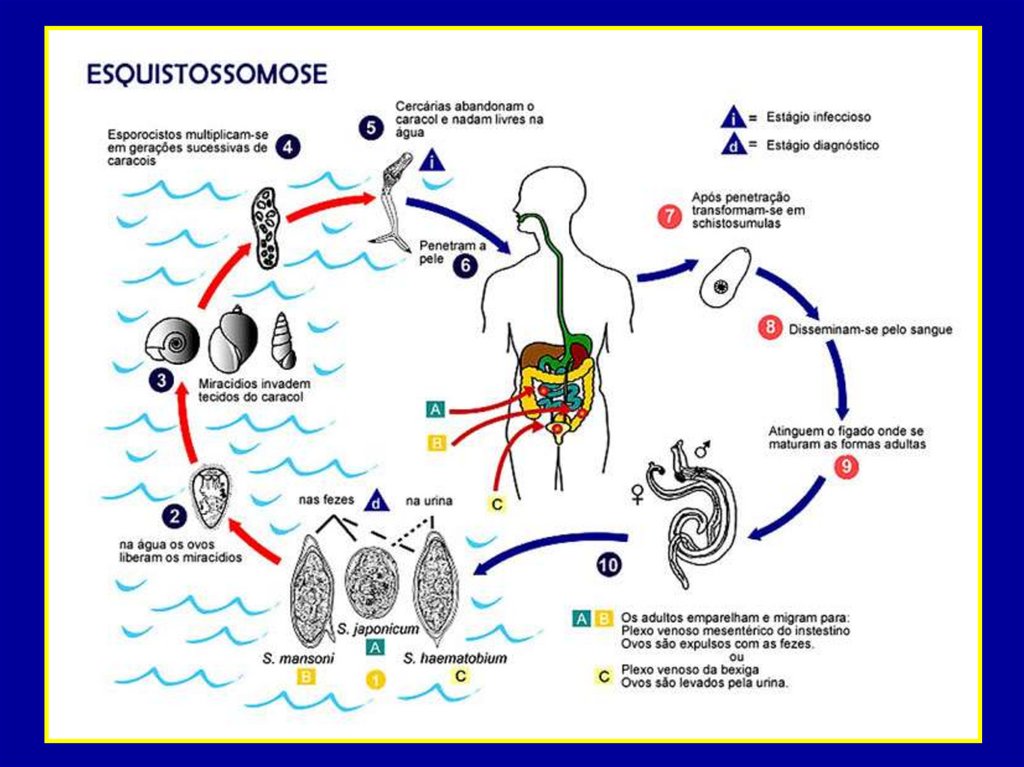
1.Eggs are excreted in human urine and feces in areas with poor
sanitation, contaminate freshwater sources.
2.
The eggs break open to release a form of the parasite called
miracidium.
3.
Freshwater snails become infested with the miracidium, which
multiply inside the snail and mature into multiple cercariae that the
snail ejects into the water.
4.
The cercariae, which survive outside a host for 48 hours, quickly
penetrate in the skin, mucous membranes of the mouth or
gastrointestinal tract.
5.
Once inside the human body, the worms penetrate the wall of the
nearest vein and travel to the liver where they grow and sexually
mature.
12.
6.Mature male and female worms
pair and migrate to the intestine or
the bladder where egg production
occurs.
One female worm may lay an
average of 200 to 2,000 eggs per
day.
Most eggs leave the blood
stream and body through the
intestine.
7. Some of the eggs are not excreted,
and can lodge in the tissues.
Presence of the eggs causes a
disease.
The highest level of prevalence and intensity of eggs - in children (10-14 years).
13.
14.
15.
ADULT PARASITES DO NOT GO OUT FROM THEBODY OF A HUMAN OR ANIMAL
From penetration of cercariae
up to the releasing of eggs
- 30-45 days
16.
Groups of risk:workers of rice and sugar plantations, irrigation systems
and fishermen.
Intensity of transmission determined by the abundance of
shellfish, their species composition and susceptibility to a
particular strain of schistosomes.
17.
IMMUNITYNatural - human immunity against schistosoma
of birds and animals.
Acquired – nonsterile, invasion is not self-limiting.
The main rison of the development of immunity - mature
parasites, products of their metabolism, membrane proteins and
eggs.
Antibodies do not destroy adults worms, but affect schistosomula,
preventing superinvasion.
Immunic complexes affect blood vessels, tissues, organs (kidney,
liver, spleen).
The most typical immunopatologic defeat – formation of
granuloma around the eggs, which has necrotic-inflammation
character.
18.
PATHOGENESIS1. Sensitization of the organism by toxic products of schistosomula and
cercariae.
2. Migration of eggs through the vessel walls of the bladder and intestine, in
the liver, lungs, brain and other organs accompanied by the development of
granulomas (inflammatory and allergic process ends fibrosis).
3. Proliferation of connective tissue of blood vessels leads to the development of
obliterating endarteritis in the liver (portal hypertension) and lung (pulmonary
heart).
Migration of eggs in the system of
portal vein promotes a proliferation
of connective tissue around the portal
vein, varicose veins of the esophagus
and development of portal hypertension
• .
19.
CLINICAL CLASSIFICATION (WHO)1. Stage of infection (invasion)
- penetration phase
- migration phase
2. Stage of maturation
3. Stage of impending invasion
4. Stage of late invasion
(complications irreversible changes)
First two stages are the same for all types of schistosoma
Incubation period - 4-16 weeks.
20.
1. Stage of infection:Penetration phase (5-6 days):
in primary infection may be asymptomatic,
in re-infections - acute dermatitis (in15 min or 1-2 days),
- itching, erythema, rash urticaria,
- weakness, insomnia, fever.
-
Migration phase (up to 2 months):
- cough, sometimes hemoptysis, asthma syndrome,
- malaise, decreased appetite, headache,
- enlarged liver and spleen,
- lymphadenopathy,
- eosinophilic infiltration in the lungs, liver, spleen, colon,
pancreas, brain,
- leukocytosis, eosinophilia, increased ESR
21.
2. Stage of maturation(Japanese sch. - 4 weeks, Mansony sch.-5 weeks,
urogenital sch. -8-10 weeks):
- parasites complet there maturation, lay eggs and reach their
habitats
Clinically: - high temperature with eosinophilia, headache,
weakness,
- loss of appetite, abdominal pain, nausea, diarrhea,
- rash,
- increased alpha-, gamma-globulin,
- «syndrome Katayama» (in Japanese sch. in europeans)
eosinophilia, splenomegaly, rash urticaria at the
absence of eggs in the stool.
22.
3.Stage of impending invasion (3-7 years):Common to all types of schistosomiasis:
- intensive production of eggs in the place of parasitizing and
discharge with urine and feces,
-development s of destructive reaction (necrosis, exudation,
eozinofilia) around the egg with subsequent proliferation,
- thrombosis and inflammation of blood vessels,
23.
Intestinal schistosomiasis:characterized by lesions of large intestine (eggs pass through the
wall), the liver and spleen.
Stage of impending invasion:
- pain in the abdomen, frequent stool with admixe of blood and
mucus, tenesmus,meteorism,
- polyps of the colon - pain, partial or total obstruction of the
bowel, weight loss,
- affection of the liver and spleen (associated with drift eggs and
granulemas) – heaviness in epigastrium, hepatosplenomegaly,
hypoproteinemia, increased ALT, anemia,
- the defeat of the spinal cord (paraplegia, pain),
- glomerulonephritis, pneumonia, bronchitis, asthma, emphysema
24.
Stage of late invasion:- Simmer’s fibrosis (fibrosis around the the portal vein)
- liver is enlarged, dense, insufficiency of liver function,
splenomegaly (cell proliferation),
- oedema of lower limbs, ascites,
- diarrhea, varicose veins of the esophagus, vascular thrombosis,
- cardiovascular insufficiency,
- polyposis of the colon,
-kidney damage (deposition of IgM, IgG),
- pulmonary hypertension (cough, syncope, tachycardia, cyanosis,
swelling),
- anaemia, lakopenia, trombopenia, hypoalbuminemia.
25.
Japanese schistosomiasis:1. The worms produce the maximum number of eggs (up to 3,000),
2. Necrosis followed by fibrosis prevails in granulemas,
3. Fibrosis of the liver is often developed,
4. Drift of eggs in the nervous system activates development of gepatotserebral
encephalopathy, acute and chronic cerebral form of psychosis,
Schistosomiasis Mekongi (like the Japanese):
-often bacteremia caused by Salmonella, which are localized on the surface
-or in the intestine of schistosomes.
26.
LABORATORY DIAGNOSTICS:1. Microscopic detection of eggs in the urine (after physical
exertion), faeces (method of thick smear by Kato),
less - in sputum, semen, liquor with a certain amount of eggs.
2. Larva-scopy – after the incubation of sediment urine or
faeces with a water detect moving miracidium.
3. Cystoscopy (determination of changes in the mucosa atrophy, pallor, thinning of the blood vessels, hyperemia,
accumulation of eggs, polyps, ulcers) with intravesical biopsy
(identification eggs) – in urogenital schistosomiasis.
4. RR-scopy (hyperemia, erosion, ulcer, papillomas) with
biopsy - in the case of intestinal schistosomiasis.
27.
5. Clinical methods – X-ray examination of the bladder,lungs, esophagus, stomach, angiography, biochemical,
and laparoscopy.
6. Immunological methods (on early and late sages) CBR, RP, ELISA and other.
5. Material of autopsy - swabs-prints.
28.
BiltricidPrasiqantel
Oxamniquine
Methrifonat
(Bilarcil)
40-60
мg\кg
In once At all schistosomiasis
15 мg\кg
2 times
(Est
Center.
Africa
15 mg\kg
(S.Аме
rica)
2days
In once
Intestinal
schistosomiasis
7,5-10
мg\кg
In once
Urogenital
schistosomiasis
29.
Niridasole(Ambilhar)
25мg\кg\d
5-7days
At all
schistosomiasis
(seldom)
Gycanton
(etrenol)
2-3 мg\кg
In once
At all
schistosomiasis
Аmoscanat
7 мg\кg in 3 Repeat in
times
7 days
(Isotyotsianat)
At all
schistosomiasis
30.
PREVENTION1. Straggle with the intermediate hosts - mollusks (chemical
method and biological methods - bacteria, fish, crabs; ecological
method - environmental change).
2. Improvement of the source of the invasion: therapy of sick
people and infected animals. At high infestation - chemotherapy
for all children.
3. Sanitary-hygienic measures on improvement of settlements
(water, sewerage, shower and other).
4. Individual prevention - protective clothing at risk groups.
5. Health education of the population (not pollute the water
with feces, not to swim and others).
6. Sanitary supervision over natural reservoirs